

Review
doi: 10.1136/gut.2005.065946.
Human pancreatic exocrine response to nutrients in health and disease
Affiliations
- PMID: 15951527
- PMCID: PMC1867805
- DOI: 10.1136/gut.2005.065946
Item in Clipboard
Review
Human pancreatic exocrine response to nutrients in health and disease
Gut.
2005 Jul.
No abstract available
Figures

Interdigestive amylase output in healthy volunteers during daytime. Enzyme output is cyclical: it is associated with intestinal motility and is higher during phases II and III compared with phase I (*p<0.05 v phase I).322
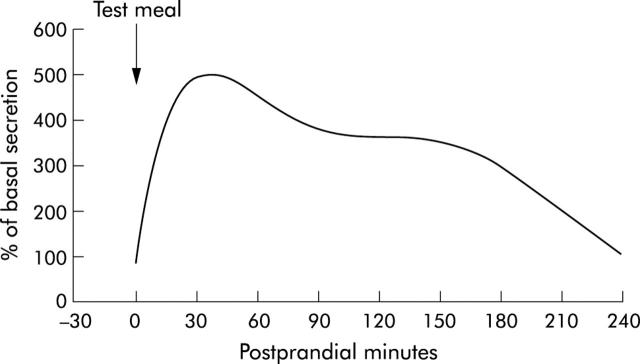
Digestive pancreatic enzyme response to a regular meal. Enzyme delivery into the duodenum increases rapidly and reaches maximal values within the first postprandial hour or even within 20–30 minutes postprandially. Following peak output, enzyme secretion decreases to almost stable secretory rates at lower levels until about 3–4 hours postprandially depending on the size of the meal. The interdigestive range is reached again at the end of the digestive period.7–13
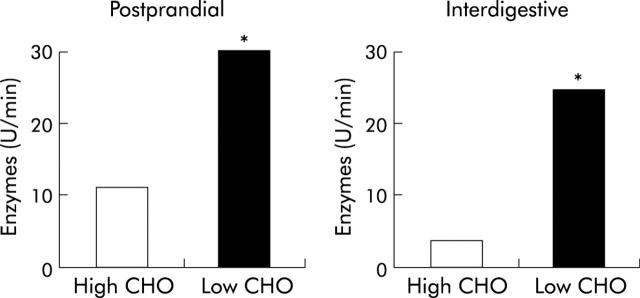
Effect of chronic ingestion of diets with varying nutrient composition in healthy volunteers. Following ingestion of a diet low in carbohydrate content (10%) and high in fat content (40%) for four weeks, postprandial enzyme output was about twice as high as following a high carbohydrate (80%), low fat (10%) diet (geometric means, ANOVA: *p<0.05). Interdigestive pancreatic enzyme output was about four times higher with the low carbohydrate, high fat diet. Thus, chronic ingestion of a high fat diet is associated with higher enzyme outputs than a carbohydrate rich diet.24
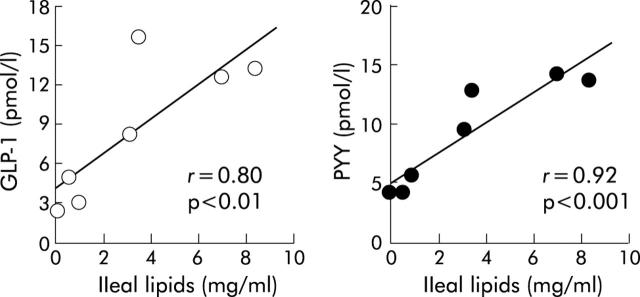
Ileal lipid exposure dose dependently releases glucagon-like peptide-1(GLP-1) and peptide YY (PYY) in healthy humans.20
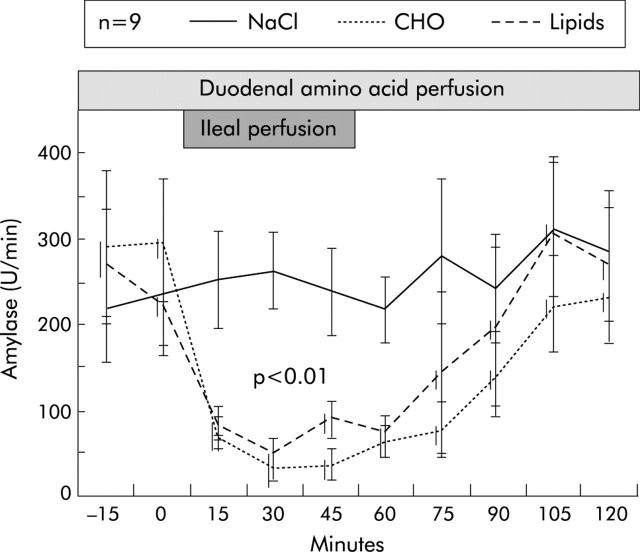
Inhibition of endogenously stimulated pancreatic enzyme secretion by ileal perfusion of carbohydrates (CHO) and lipids in healthy humans.17
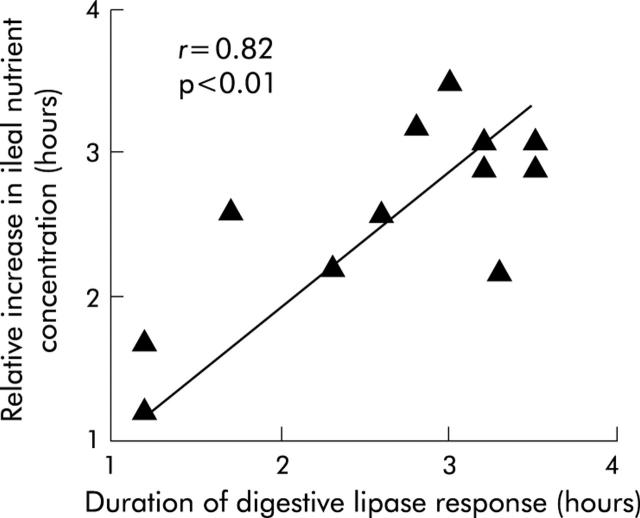
Correlation between the duration of digestive lipase secretion and the time of the relative increase in ileal nutrient concentration in healthy humans.18
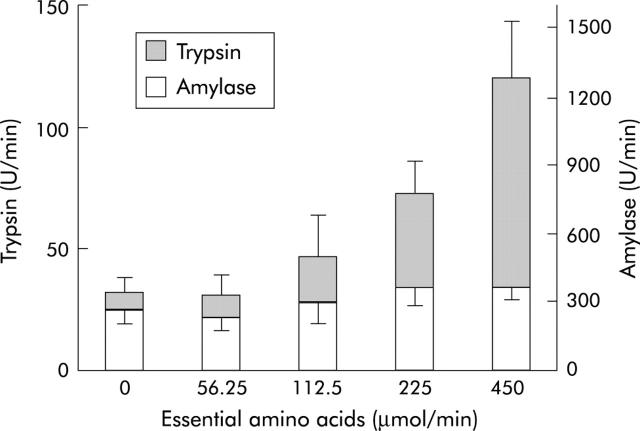
Differential effects of graded duodenal nutrient perfusion on protease and amylase outputs in healthy humans. Essential amino acids at doses up to 450 µg/min dose dependently stimulated trypsin but had no effect on amylase output (*p<0.05).49
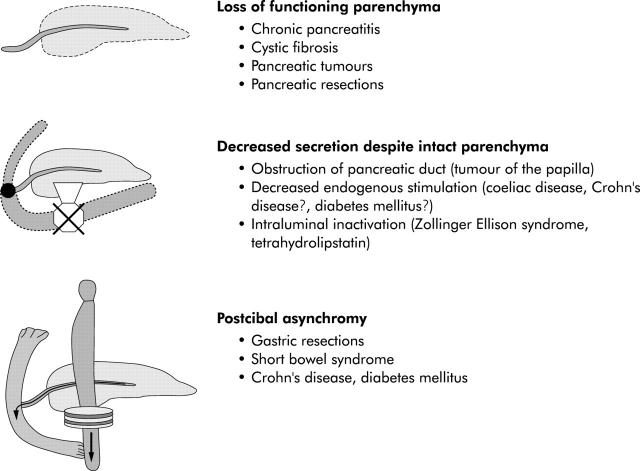
Pathomechanisms causing intraluminal pancreatic enzyme deficiency.
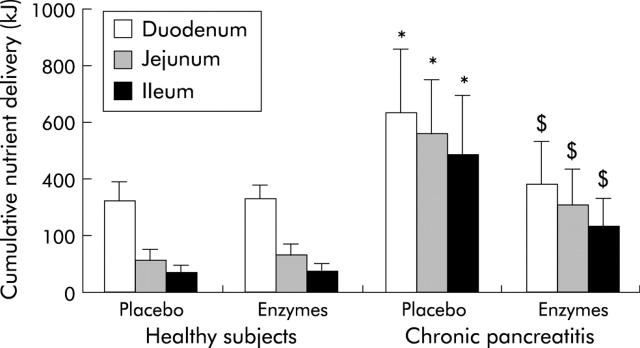
Nutrient malabsorption with and without enzyme supplementation in healthy subjects (n = 14) and patients with chronic pancreatitis (n = 12).104
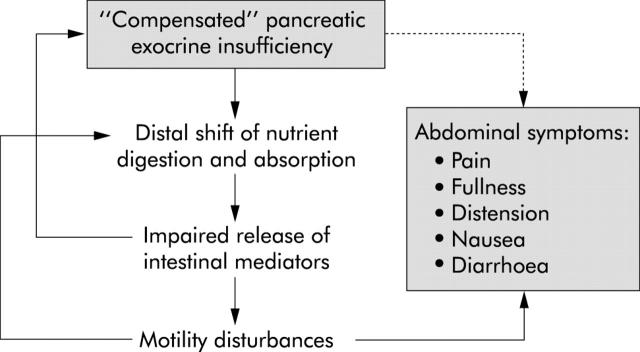
Potential pathophysiological role of "compensated" pancreatic exocrine insufficiency for abdominal symptoms: in patients with mildly to moderately decreased exocrine function a distal shift of nutrient digestion and absorption may lead to impaired release of intestinal mediators. This, in turn may cause motility disturbances inducing abdominal symptoms and it may aggravate exocrine insufficiency. Accordingly, abdominal symptoms would not be a consequence of increased loss of nutrients but of a disturbance of the integrated regulation of gastrointestinal secretory and motor functions.
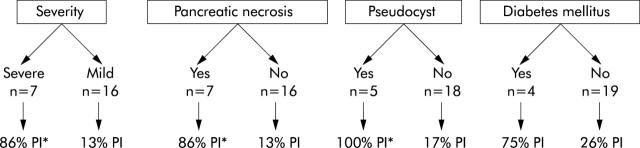
Incidence of pancreatic exocrine insufficiency (PI) in 23 patients recovering from acute pancreatitis depending on severity of disease and presence of complications.169 *p = 0.002 mild v severe or absence v presence of symptoms.
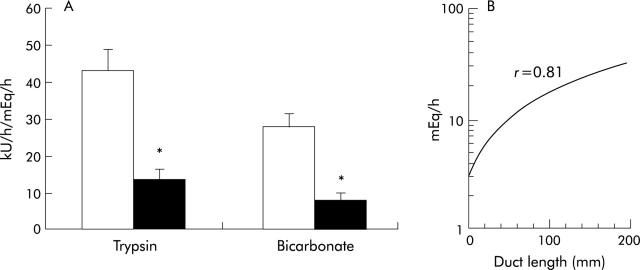
(A) Trypsin and bicarbonate response to CCK are significantly decreased in patients with pancreatic cancer (n = 17, black bars) compared with controls (n = 17, open bars). (B) Bicarbonate output in response to CCK is significantly correlated with (remaining) length of pancreatic duct for combined pancreatic cancer and control groups (*p<0.05).171
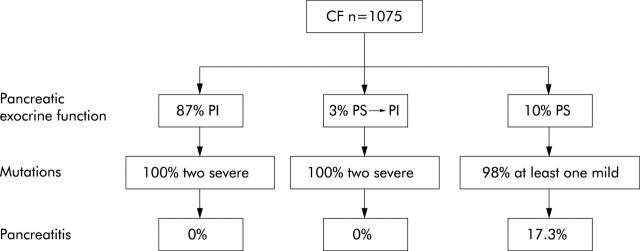
About 10% of patients with cystic fibrosis remain pancreatic sufficient (PS), 3% develop pancreatic insufficiency during the course of the disease (PS → PI) and 87% show pancreatic exocrine insufficiency at diagnosis (PI). All patients with PI or PS → PI in whom complete genotype analysis could be performed showed severe CFTR gene mutations on both alleles. By contrast, almost all patients with PS had at least one mild mutation. Only patients with PS appear to be at risk of developing (recurrent) acute pancreatitis.183
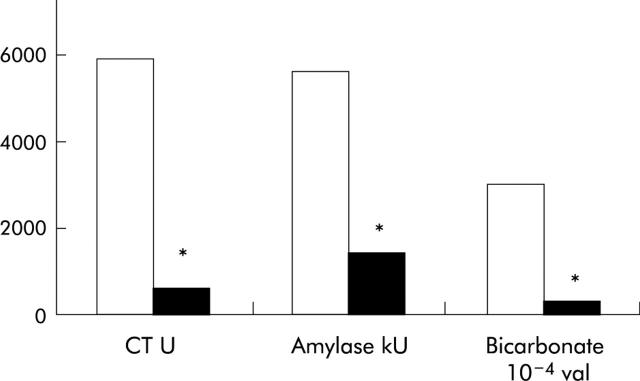
Median enzyme and bicarbonate output in patients before (open bars) and three months after (black bars) total gastrectomy due to gastric cancer. Preoperatively, all patients had normal pancreatic exocrine function. Median output of all parameters in response to direct stimulation by secretin and cerulein was markedly and significantly decreased postoperatively (*p<0.01).98
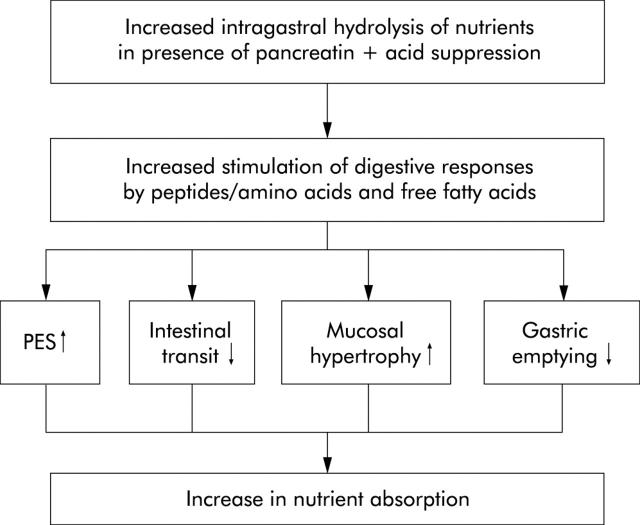
Theoretical effect of pancreatic enzyme supplementation in short bowel syndrome (PES, pancreatic enzyme secretion). Application of unprotected pancreatic enzymes together with gastric acid suppression therapy should enable gastric digestion of nutrients with increased delivery of digestive products to the small bowel. Because of the superior stimulatory capacity of peptides, amino acids, and free fatty acids compared with macronutrients, conditions for nutrient absorption should be improved by increased endogenous pancreatic enzyme secretion, delayed gastric emptying, and small intestinal transit as well as mucosal hypertrophy.
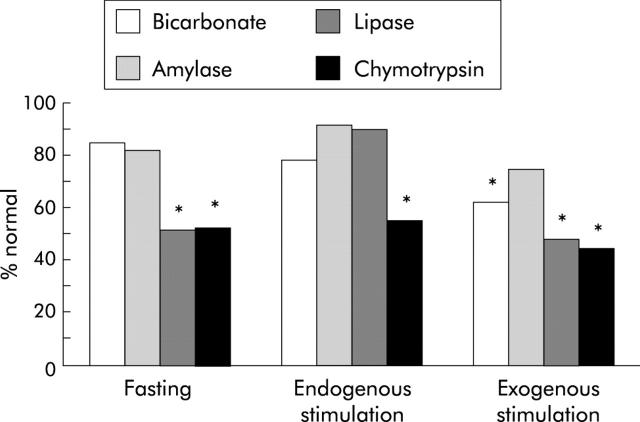
Exocrine pancreatic insufficiency in type I diabetes mellitus: differential susceptibility of individual enzymes to endogenous and exogenous stimulation. Amylase output was normal in the interdigestive state, during moderate endogenous and maximal exogenous stimulation. Diminished fasting lipase output increased regularly in response to endogenous but not to exogenous stimulation. Chymotrypsin output was most susceptible and was decreased under all experimental conditions.262
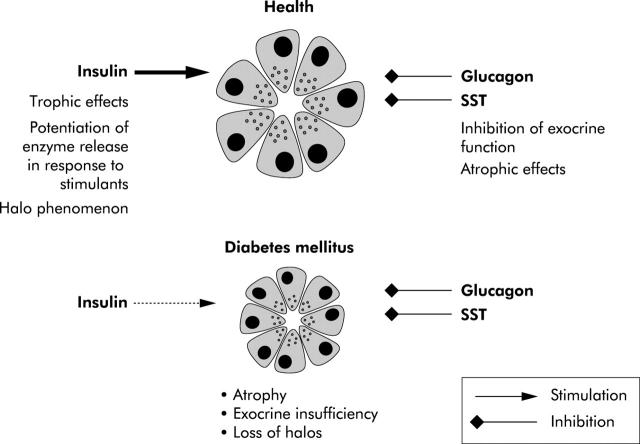
Imbalance of stimulatory and inhibitory pancreatic islet hormones in diabetes mellitus.273
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical