

Spatial analysis of lung, colorectal, and breast cancer on Cape Cod: an application of generalized additive models to case-control data
- PMID: 15955253
- PMCID: PMC1183231
- DOI: 10.1186/1476-069X-4-11
Spatial analysis of lung, colorectal, and breast cancer on Cape Cod: an application of generalized additive models to case-control data
Abstract
Background: The availability of geographic information from cancer and birth defect registries has increased public demands for investigation of perceived disease clusters. Many neighborhood-level cluster investigations are methodologically problematic, while maps made from registry data often ignore latency and many known risk factors. Population-based case-control and cohort studies provide a stronger foundation for spatial epidemiology because potential confounders and disease latency can be addressed.
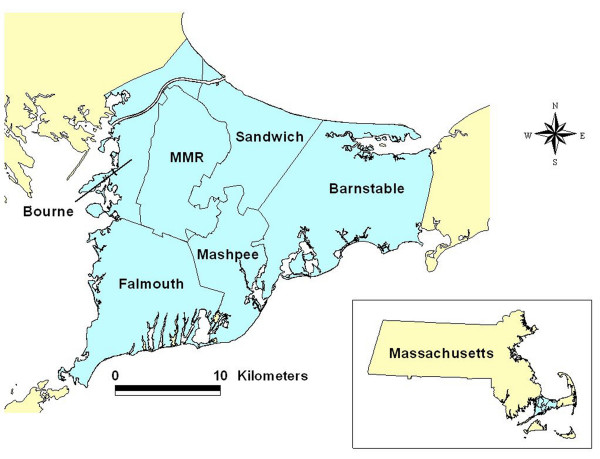
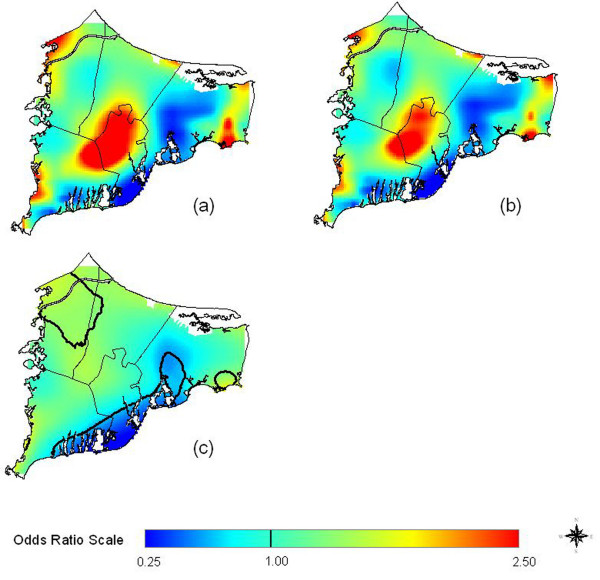
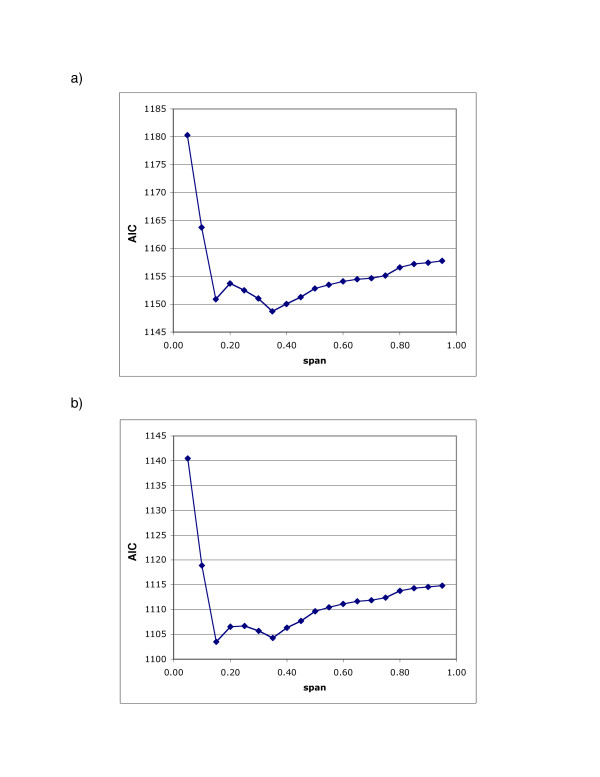
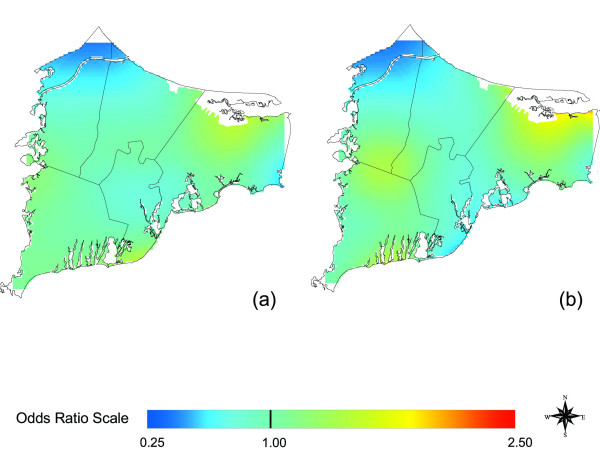
Methods: We investigated the association between residence and colorectal, lung, and breast cancer on upper Cape Cod, Massachusetts (USA) using extensive data on covariates and residential history from two case-control studies for 1983-1993. We generated maps using generalized additive models, smoothing on longitude and latitude while adjusting for covariates. The resulting continuous surface estimates disease rates relative to the whole study area. We used permutation tests to examine the overall importance of location in the model and identify areas of increased and decreased risk.
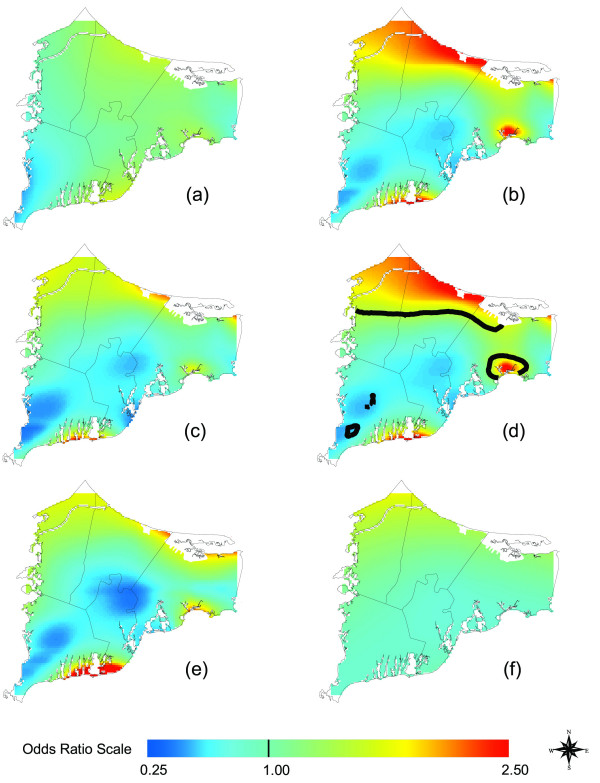
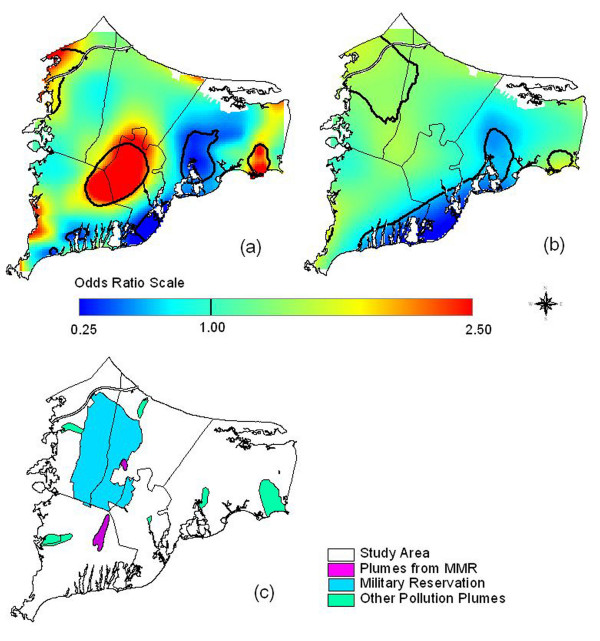
Results: Maps of colorectal cancer were relatively flat. Assuming 15 years of latency, lung cancer was significantly elevated just northeast of the Massachusetts Military Reservation, although the result did not hold when we restricted to residences of longest duration. Earlier non-spatial epidemiology had found a weak association between lung cancer and proximity to gun and mortar positions on the reservation. Breast cancer hot spots tended to increase in magnitude as we increased latency and adjusted for covariates, indicating that confounders were partly hiding these areas. Significant breast cancer hot spots were located near known groundwater plumes and the Massachusetts Military Reservation.
Discussion: Spatial epidemiology of population-based case-control studies addresses many methodological criticisms of cluster studies and generates new exposure hypotheses. Our results provide evidence for spatial clustering of breast cancer on upper Cape Cod. The analysis suggests further investigation of the potential association between breast cancer and pollution plumes based on detailed exposure modeling.
Figures



References
-
- Rothman K. A sobering start for the cluster busters' conference. Am J Epidemiol. 1990;132:S6–S13. - PubMed
-
- Polissar L. The effect of migration on comparison of disease rates in geographic studies in the United States. Am J Epidemiol. 1980;111:175–182. - PubMed
-
- Neutra RR. Counterpoint from a cluster buster. Am J Epidemiol. 1990;132:1–8. - PubMed
-
- Wartenberg D. Investigating disease clusters: Why, when, how? J Royal Statist Soc A. 2001;164:13–22. doi: 10.1111/1467-985X.00181. - DOI
-
- Aschengrau A, Ozonoff D. Upper Cape Cancer Incidence Study Final Report. Boston: Massachusetts Department of Public Health; 1992.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
