

Stent-assisted angioplasty of symptomatic intracranial vertebrobasilar artery stenosis: feasibility and follow-up results
- PMID: 15956503
- PMCID: PMC8149083
Stent-assisted angioplasty of symptomatic intracranial vertebrobasilar artery stenosis: feasibility and follow-up results
Abstract
Background and purpose: The natural history of symptomatic, untreated posterior circulation stenosis is dismal, with many patients experiencing significant morbidity or mortality. The purpose of this study was to evaluate the feasibility and results of stent-assisted angioplasty of symptomatic intracranial vertebrobasilar artery stenosis.
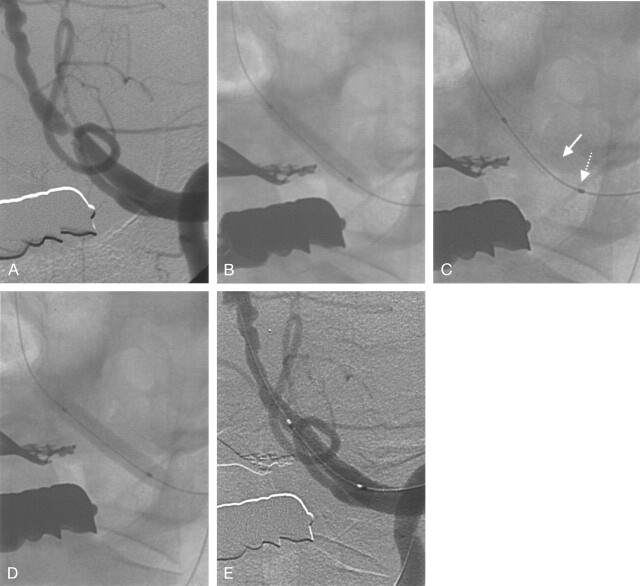
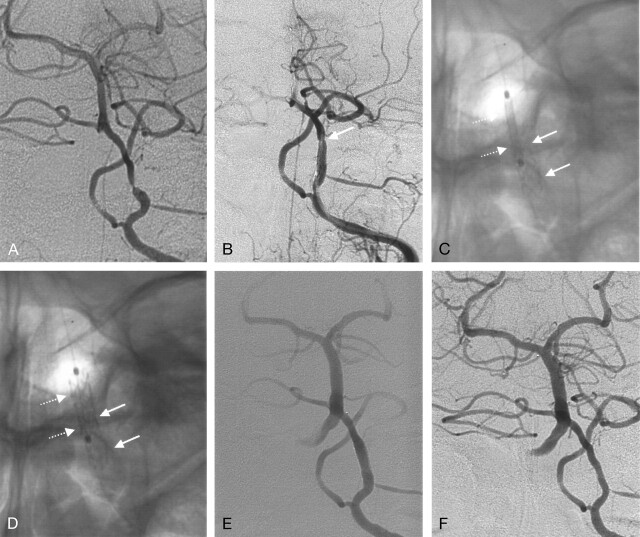
Methods: We reviewed the imaging findings and medical records of 17 consecutive patients who were treated with stent-assisted angioplasty for medically refractory vertebrobasilar artery stenosis. The location of the lesion, degree of stenosis, procedure-related complications, and clinical and short- and long-term angiographic results were assessed.
Results: The population included 17 cases (10 men, seven women; age range, 51-74 years; mean, 64 years). The locations of the lesions were intracranial vertebral artery (n = 13) and basilar artery (n = 6). The mean degree of stenosis decreased from 76.1 +/- 14.6% before stent-assisted angioplasty to 1.3 +/- 2.8% (P < .05) after the procedure. Acute in-stent thrombosis developed in one case (6%, Mori type B lesion), which was successfully treated with intraarterial abciximab infusion and angioplasty. Another patient (6%, Mori type C lesion) developed immediate postprocedural transient diplopia and ataxia, which gradually resolved. No other patient showed symptoms related to the vertebrobasilar artery lesion at follow-up. No significant restenosis was observed at short-term (five patients; follow-up range, 0.5-6 months; mean, 4.3 months) or long-term (six patients; follow-up range, 12-41 months; mean, 21 months) angiographic follow-up.
Conclusion: Stent-assisted angioplasty is a feasible treatment method for vertebrobasilar artery stenosis. The patency of the stent-assisted angioplasty seems to be preserved in the long-term, with good clinical outcome.
Figures
References
-
- Moufarrij NA, Little JR, Furlan AJ, Leatherman JR, Williams GW. Basilar and distal vertebral artery stenosis: long-term follow-up. Stroke 1986;17:938–942 - PubMed
-
- Ausman JI, Shrontz CE, Pearce JE, Diaz FG, Crecelius JL. Vertebrobasilar insufficiency: a review. Arch Neurol 1985;42:803–808 - PubMed
-
- The Warfarin-Aspirin Symptomatic Intracranial Disease (WASID) Study Group. Prognosis of patients with symptomatic vertebral or basilar artery stenosis. Stroke 1998;29:1389–1392 - PubMed
-
- Connors JJ 3rd, Wojak JC. Percutaneous transluminal angioplasty for intracranial atherosclerotic lesions: evolution of technique and short-term results. J Neurosurg 1999;91:415–423 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources