

Neurologic complications after particle embolization of intracranial meningiomas
- PMID: 15956508
- PMCID: PMC8149084
Neurologic complications after particle embolization of intracranial meningiomas
Abstract
Background and purpose: Preoperative embolization of meningiomas is frequently used to facilitate surgery and to reduce intraoperative blood loss. The purpose of this study was to evaluate the frequency of procedure-related neurologic complications during and after particle embolization of intracranial meningiomas.
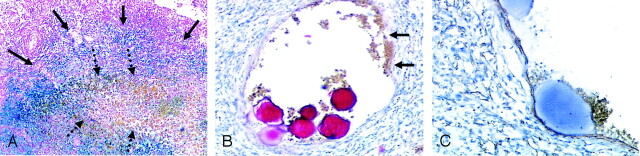
Methods: Between 1996 and 2004, 185 consecutive patients underwent particle embolization of an intracranial meningioma. Devascularization was performed by means of superselective probing of the tumor-feeding vessels and ensuing free-flow embolization with spherical particles. All procedures were performed with systemic heparinization.
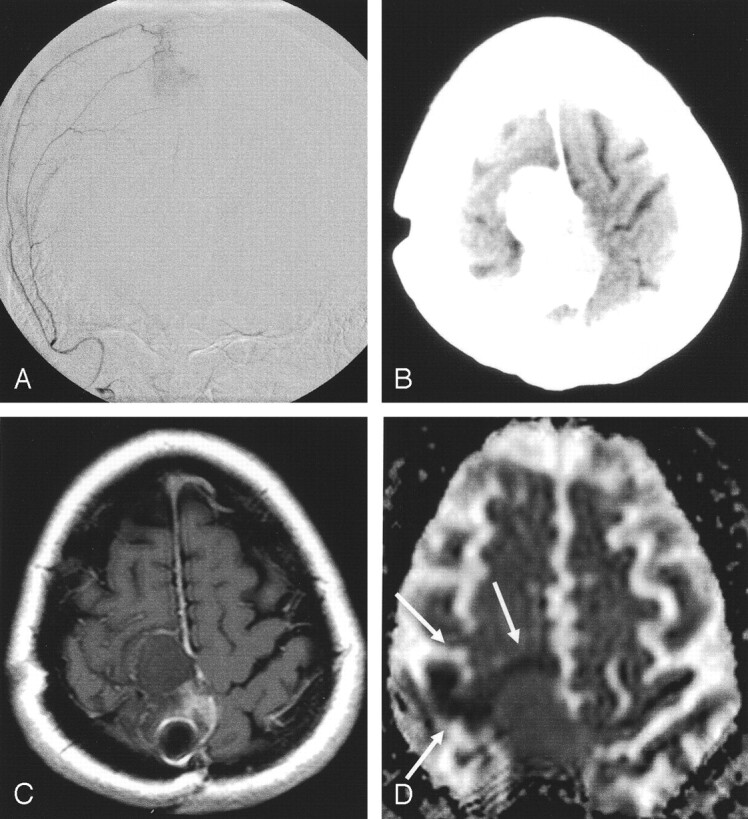
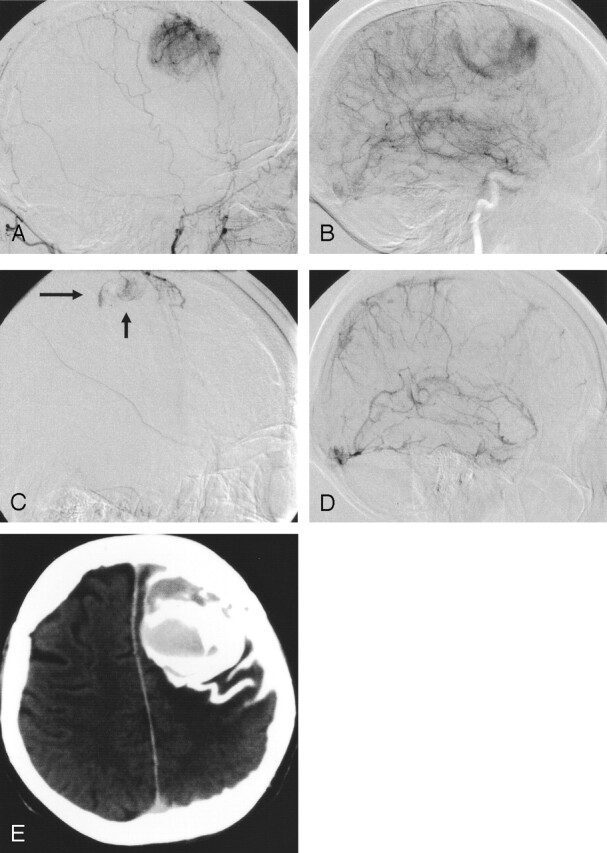
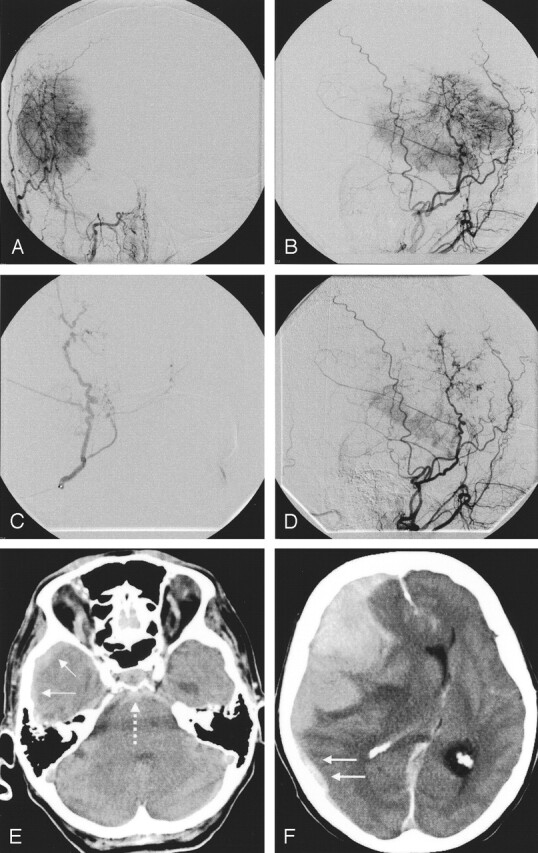
Results: Six patients (3.2%) had ischemic events with neurologic deficit. Two had amaurosis, and four patients presented with hemiparesis. Hemorrhage occurred in six patients (3.2%). In five of these patients, rapid microsurgical tumor removal resulted in a favorable outcome without persistent neurologic deficit. In one patient, massive intratumoral, subarachnoid, and subdural hemorrhage was lethal.
Conclusion: Particle embolization of meningiomas is associated with a substantial risk of ischemic and hemorrhagic events. The individual risk-to-benefit ratio of embolization should be thoroughly considered.
Figures
Similar articles
-
Preoperative embolization of meningiomas: comparison of superselective and subselective techniques.J Formos Med Assoc. 1998 Mar;97(3):153-8. J Formos Med Assoc. 1998. PMID: 9549263
-
Complications of particle embolization of meningiomas: frequency, risk factors, and outcome.AJNR Am J Neuroradiol. 2010 Jan;31(1):152-4. doi: 10.3174/ajnr.A1754. Epub 2009 Sep 3. AJNR Am J Neuroradiol. 2010. PMID: 19729535 Free PMC article.
-
Controversies in the role of preoperative embolization in meningioma management.Neurosurg Focus. 2013 Dec;35(6):E17. doi: 10.3171/2013.9.FOCUS13351. Neurosurg Focus. 2013. PMID: 24289125 Review.
-
Embolization of meningiomas: comparison of safety between calibrated microspheres and polyvinyl-alcohol particles as embolic agents.AJNR Am J Neuroradiol. 2013 Apr;34(4):727-9. doi: 10.3174/ajnr.A3311. Epub 2012 Oct 18. AJNR Am J Neuroradiol. 2013. PMID: 23079408 Free PMC article. Clinical Trial.
-
Strategic and Technical Considerations for the Endovascular Embolization of Intracranial Meningiomas.Neurosurg Clin N Am. 2016 Apr;27(2):155-66. doi: 10.1016/j.nec.2015.11.005. Epub 2016 Feb 18. Neurosurg Clin N Am. 2016. PMID: 27012380 Review.
Cited by
-
Head, neck, and brain tumor embolization guidelines.J Neurointerv Surg. 2012 Jul;4(4):251-5. doi: 10.1136/neurintsurg-2012-010350. Epub 2012 Apr 26. J Neurointerv Surg. 2012. PMID: 22539531 Free PMC article. Review.
-
Preoperative embolization of hypervascular pediatric brain tumors: evaluation of technical safety and outcome.Childs Nerv Syst. 2013 Nov;29(11):2043-9. doi: 10.1007/s00381-013-2128-2. Epub 2013 May 4. Childs Nerv Syst. 2013. PMID: 23644575
-
The role of preoperative angiography in the management of giant meningiomas associated to vascular malformation.Surg Neurol Int. 2015 Jun 29;6:114. doi: 10.4103/2152-7806.159490. eCollection 2015. Surg Neurol Int. 2015. PMID: 26167366 Free PMC article.
-
Preoperative onyx embolization of meningiomas fed by the ophthalmic artery: a case series.AJNR Am J Neuroradiol. 2011 Oct;32(9):1762-6. doi: 10.3174/ajnr.A2591. Epub 2011 Aug 11. AJNR Am J Neuroradiol. 2011. PMID: 21835949 Free PMC article.
-
Preoperative embolization of intracranial meningiomas using n-butyl cyanoacrylate.Neuroradiology. 2015 Jul;57(7):713-9. doi: 10.1007/s00234-015-1521-9. Epub 2015 Apr 7. Neuroradiology. 2015. PMID: 25845812
References
-
- Manelfe C, Guiraud B, David J, et al. Embolisation par catherterisme des meningiomes intracranienes. Rev Neurol 1973;128:339–351 - PubMed
-
- Hieshima GB, Everhart FR, Mehringer CM, et al. Preoperative embolization of meningiomas. Surg Neurol 1980;14:119–127 - PubMed
-
- Rosen CL, Ammerman JM, Sekhar LN, Bank WO. Outcome analysis of preoperative embolization in cranial base surgery. Acta Neurochir (Wien) 2002;144:1157–1164 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical