

Diffusion-weighted and fluid-attenuated inversion recovery imaging in Creutzfeldt-Jakob disease: high sensitivity and specificity for diagnosis
- PMID: 15956529
- PMCID: PMC8149066
Diffusion-weighted and fluid-attenuated inversion recovery imaging in Creutzfeldt-Jakob disease: high sensitivity and specificity for diagnosis
Abstract
Background and purpose: Abnormalities on diffusion-weighted images (DWIs) and fluid-attenuated inversion recovery (FLAIR) images are reported in Creutzfeldt-Jakob disease (CJD). To our knowledge, no large study has been conducted to determine the sensitivity and specificity of DWI and FLAIR imaging for diagnosing CJD.
Methods: Two neuroradiologists, blinded to diagnosis, retrospectively evaluated DWI and FLAIR images from 40 patients with probable or definite CJD and 53 control subjects with other forms of dementia and rated the likelihood of CJD on the basis of the imaging findings.
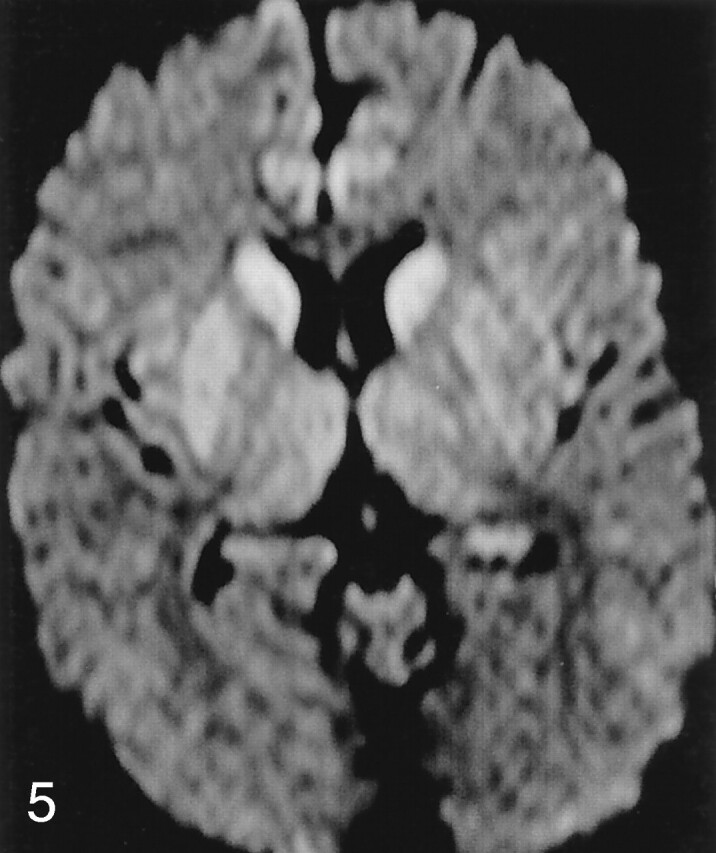
Results: DWI and FLAIR imaging was 91% sensitive, 95% specific, and 94% accurate for CJD. Interrater reliability was high (kappa = 0.93). Sensitivity was higher for DWI than FLAIR imaging. Abnormalities involved cortex and deep gray matter (striatum and/or thalamus) in 68% of patients with CJD, cortex alone in 24%, and deep gray matter alone in 5%. The most typical and specific patterns were corresponding hyperintensity on both FLAIR images and DWIs confined to the gray matter in the cortex, striatum, medial and/or posterior thalamus, or a combination of these areas. Narrow-window soft-copy review of artifact-free DWIs and FLAIR images and recognition of the normal variation in cortical signal intensity proved critical for successful differentiation of CJD from other dementias.
Conclusion: Because specific patterns of abnormality on DWI and FLAIR images are highly sensitive and specific for CJD, these sequences should be performed whenever CJD is suspected.
Figures









References
-
- Geschwind MD, Jay C. Alzheimer’s Disease and Other Primary Dementias. In: Harrison’s Principles of Internal Medicine. Bird T, ed. McGraw Hill,2003. :2391–2398
-
- World Health Organization. Global surveillance, diagnosis, and therapy of human transmissible spongiform encephalopathies: report of a WHO consultation. In: Global Surveillance, Diagnosis, and Therapy of Human Transmissible Spongiform Encephalopathies. Geneva: World Health Organization;1998. :1–29
-
- Zerr I, Pocchiari M, Collins S, et al. Analysis of EEG and CSF 14-3-3 proteins as aids to the diagnosis of Creutzfeldt-Jakob disease. Neurology 2000;55:811–815 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical