

Prevalence and clinical significance of systolic impairment in hypertrophic cardiomyopathy
- PMID: 15958362
- PMCID: PMC1768999
- DOI: 10.1136/hrt.2003.031161
Prevalence and clinical significance of systolic impairment in hypertrophic cardiomyopathy
Abstract
Objectives: To determine the frequency of systolic impairment (SI) and its impact on the natural history of hypertrophic cardiomyopathy (HCM).
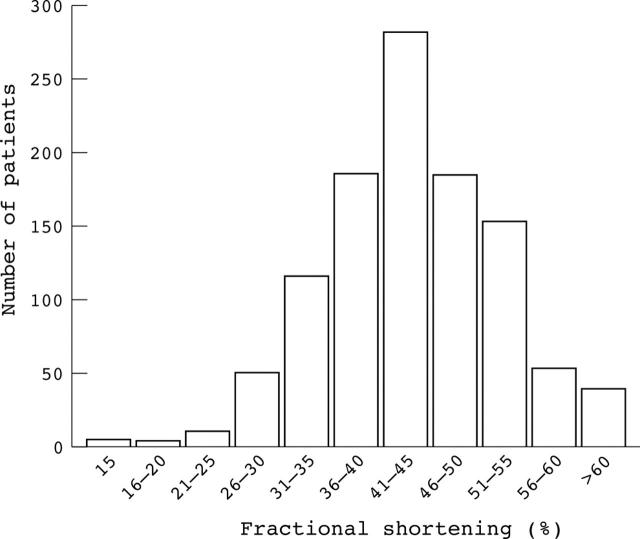
Methods: 1080 patients (mean (SD) age 43 (15) years, 660 men) with HCM were evaluated. Initial assessment included history, examination, 48 hour Holter monitoring, cardiopulmonary exercise testing, and echocardiography; SI was defined as a fractional shortening (FS) < or = 25%. Survival data were collected at clinic visits or by direct communication with patients and their general practitioners. The results of serial echocardiography in 462 patients with normal FS at presentation are also reported.
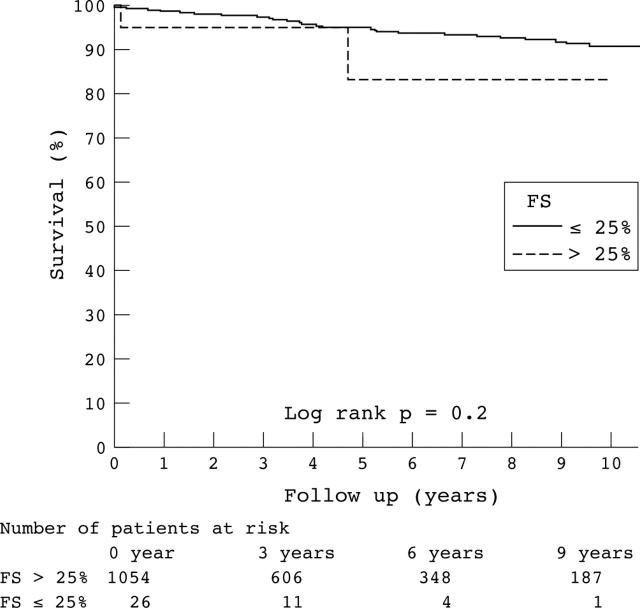
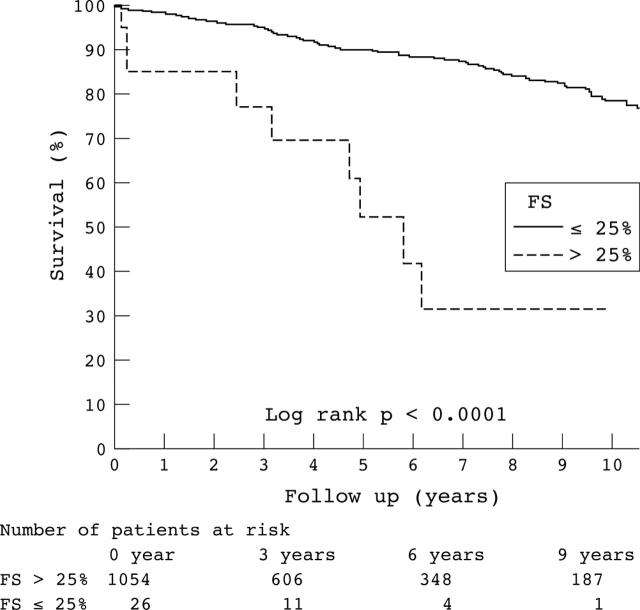
Results: 26 (2.4%) patients (49 (14) years, 18 men) had SI at the initial visit. During follow up (58 (49) months), nine (34.6%) died or underwent cardiac transplantation compared with 108 (10.2%) patients with normal FS (p = 0.01). Five year survival from death (any cause) or transplantation was 90.1% (95% confidence interval (CI) 87.8 to 92.4) in patients with normal systolic function versus 52.4% (95% CI 25.2 to 79.6, p < 0.0001) in patients with SI. In patients who underwent serial echocardiography, 22 (4.8%, aged 41 (15) years) developed SI over 66 (40) months; the annual incidence of SI was 0.87% (95% CI 0.54 to 1.31). On initial evaluation patients who developed SI had a higher frequency of syncope (67 (15.2%) v 10 (45.5%) of those who did not develop SI, p = 0.001), non-sustained ventricular tachycardia (91 (20.6%) v 11 (50%), p = 0.002), and an abnormal blood pressure response on exercise (131 (29.7%) v 15 (68.2%), p = 0.001). Patients with SI had greater wall thinning (p = 0.001), left ventricular cavity enlargement (p < 0.0005), and deterioration in New York Heart Association functional class (p = 0.001) during follow up. Thirteen (59.1%) patients who progressed to SI died or underwent transplantation compared with 38 (8.6%) patients who maintained normal systolic function.
Conclusions: SI is an infrequent complication of HCM but, when present, is associated with a poor prognosis.
Figures
References
-
- Spirito P, Maron BJ, Bonow RO, et al. Occurrence and significance of progressive left ventricular wall thinning and relative cavity dilatation in hypertrophic cardiomyopathy. Am J Cardiol 1987;60:123–9. - PubMed
-
- Hina K, Kusachi S, Iwasaki K, et al. Progression of left ventricular enlargement in patients with hypertrophic cardiomyopathy: incidence and prognostic value. Clin Cardiol 1993;16:403–7. - PubMed
-
- Shirani J, Maron BJ, Cannon RO III, et al. Clinicopathologic features of hypertrophic cardiomyopathy managed by cardiac transplantation. Am J Cardiol 1993;72:434–40. - PubMed
-
- Suwa M, Hirota Y, Nakayama Y, et al. [Natural course of hypertrophic cardiomyopathy: clinical, hemodynamic and echocardiographic features in the end stage]. J Cardiol Suppl 1987;16:65–78. - PubMed
-
- Richardson P, McKenna W, Bristow M, et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology task force on the definition and classification of cardiomyopathies. Circulation 1996;93:841–2. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources