

The CP stent--short, long, covered--for the treatment of aortic coarctation, stenosis of pulmonary arteries and caval veins, and Fontan anastomosis in children and adults: an evaluation of 60 stents in 53 patients
- PMID: 15958369
- PMCID: PMC1768992
- DOI: 10.1136/hrt.2004.040071
The CP stent--short, long, covered--for the treatment of aortic coarctation, stenosis of pulmonary arteries and caval veins, and Fontan anastomosis in children and adults: an evaluation of 60 stents in 53 patients
Abstract
Objective: To evaluate the feasibility and usefulness of the Cheatham platinum (CP) stent in a broad spectrum of lesions.
Methods: Retrospective analysis of 60 implanted CP stents (11-80 mm lengths, 12 covered) between September 2001 and March 2004.
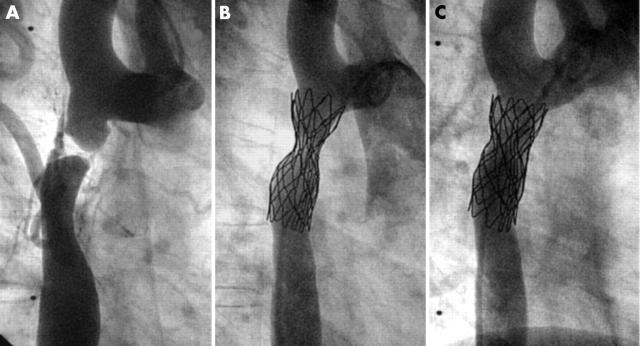
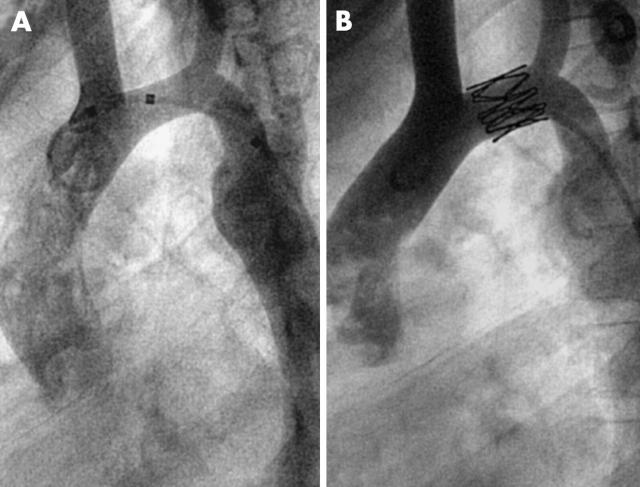
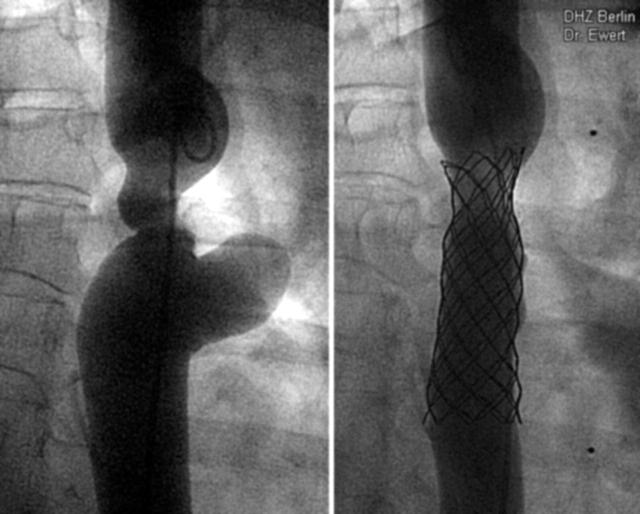
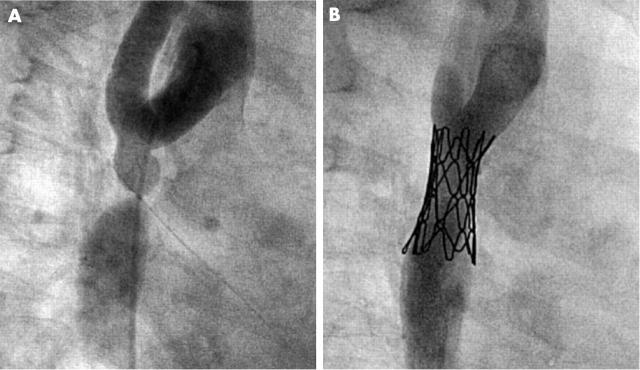
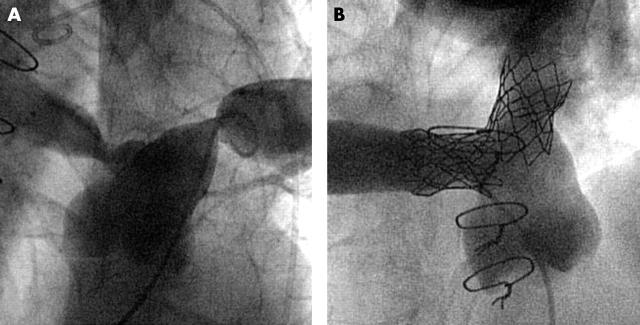
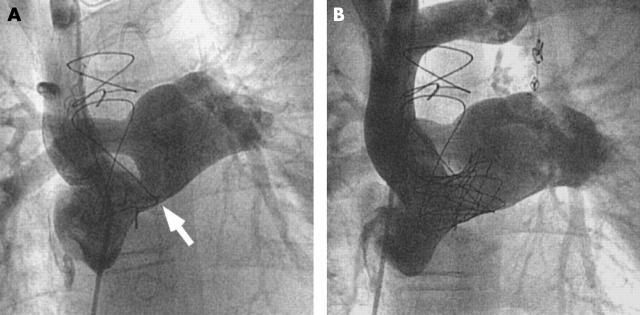
Patients: 53 patients aged 2.5-68 years (median 17 years). Body weight ranged from 12-95 kg (median 52 kg). Thirty six patients had aortic (re)coarctation; seven of them had functionally interrupted aortic arches. Thirteen patients had pulmonary artery stenosis and four had stenosis of caval veins or conduits in a total cavopulmonary connection (TCPC).
Results: Arterial pressure gradients dropped from 33 mm Hg (range 20-80 mm Hg) to 5 mm Hg (range 0-10 mm Hg) and pressure gradients in TCPC or caval veins dropped from 4 mm Hg (range 4-20 mm Hg) to 0 mm Hg (range 0-3 mm Hg). All stents were placed in the target lesion without complications. Three stent fractures without clinical instability were noted.
Conclusions: The CP stent is suitable for the treatment of vessel stenosis in congenital heart diseases from childhood to adulthood. Whether these good results will be stable in the long term needs to be investigated.
Figures
Similar articles
-
Early and mid-term results with the Growth Stent--a possible concept for transcatheter treatment of aortic coarctation from infancy to adulthood by stent implantation?Catheter Cardiovasc Interv. 2008 Jan 1;71(1):120-6. doi: 10.1002/ccd.21397. Catheter Cardiovasc Interv. 2008. PMID: 18098214
-
Covered Cheatham-platinum stents for aortic coarctation: early and intermediate-term results.J Am Coll Cardiol. 2006 Apr 4;47(7):1457-63. doi: 10.1016/j.jacc.2005.11.061. Epub 2006 Mar 20. J Am Coll Cardiol. 2006. PMID: 16580536
-
Covered stents in patients with complex aortic coarctations.Am Heart J. 2007 Oct;154(4):795-800. doi: 10.1016/j.ahj.2007.06.018. Am Heart J. 2007. PMID: 17893011
-
Anatomy of coarctation, hypoplastic and interrupted aortic arch: relevance to interventional/surgical treatment.Expert Rev Cardiovasc Ther. 2007 Sep;5(5):871-80. doi: 10.1586/14779072.5.5.871. Expert Rev Cardiovasc Ther. 2007. PMID: 17867917 Review.
-
Surgery is the best treatment for primary coarctation in the majority of cases.J Cardiovasc Med (Hagerstown). 2007 Jan;8(1):50-6. doi: 10.2459/01.JCM.0000247436.05194.c7. J Cardiovasc Med (Hagerstown). 2007. PMID: 17255817 Review.
Cited by
-
Use of Zephyr stent in congenital heart diseases: A single-center study.Ann Pediatr Cardiol. 2023 Jul-Aug;16(4):276-281. doi: 10.4103/apc.apc_78_23. Epub 2024 Jan 5. Ann Pediatr Cardiol. 2023. PMID: 38343503 Free PMC article.
-
Use of covered stents to treat coarctation of the aorta.Korean Circ J. 2009 Jul;39(7):261-3. doi: 10.4070/kcj.2009.39.7.261. Epub 2009 Jul 28. Korean Circ J. 2009. PMID: 19949609 Free PMC article.
-
Single-stage endovascular management of complicated thoracic aorta coarctation concurrent with aortic arch aneurysm using a novel fenestration device.J Thorac Dis. 2018 Apr;10(4):2474-2480. doi: 10.21037/jtd.2018.03.162. J Thorac Dis. 2018. PMID: 29850155 Free PMC article.
-
Cheatham-Platinum stent implantation for pulmonary artery stenosis in children and adolescents: immediate and mid-term outcome.World J Pediatr. 2010 Nov;6(4):337-41. doi: 10.1007/s12519-010-0233-9. Epub 2010 Nov 16. World J Pediatr. 2010. PMID: 21080145
-
Early and late outcome of covered and non-covered stents in the treatment of coarctation of aorta- A single centre experience.Indian Heart J. 2020 Jul-Aug;72(4):278-282. doi: 10.1016/j.ihj.2020.06.012. Epub 2020 Jul 2. Indian Heart J. 2020. PMID: 32861383 Free PMC article.
References
-
- O’Laughlin MP, Perry SB, Lock JE, et al. Use of endovascular stents in congenital heart disease. Circulation 1991;83:1923–39. - PubMed
-
- O’Laughlin MP, Slack MC, Grifka RG, et al. Implantation and intermediate-term follow-up of stents in congenital heart disease. Circulation 1993;88:605–14. - PubMed
-
- Schaffer AI. Coarctation hypertension is renovascular, modified by ambulation: coarctation hypertension renovascular variant. J Clin Hypertens 1986;2:69–78. - PubMed
-
- Okubo M, Benson LN. Intravascular and intracardiac stents used in congenital heart disease. Curr Opin Cardiol 2001;16:84–91. - PubMed
-
- Rutledge JM, Mullins CE, Nihill MR, et al. Initial experience with intratherapeutics IntraStent DoubleStrut LD stents in patients with congenital heart defects. Catheter Cardiovasc Interv 2002;56:541–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous