

"Light" versus "classic" laser treatment for clinically significant diabetic macular oedema
- PMID: 15965168
- PMCID: PMC1772712
- DOI: 10.1136/bjo.2004.051060
"Light" versus "classic" laser treatment for clinically significant diabetic macular oedema
Abstract
Aim: To compare the effectiveness of "light" versus "classic" laser photocoagulation in diabetic patients with clinically significant macular oedema (CSMO).
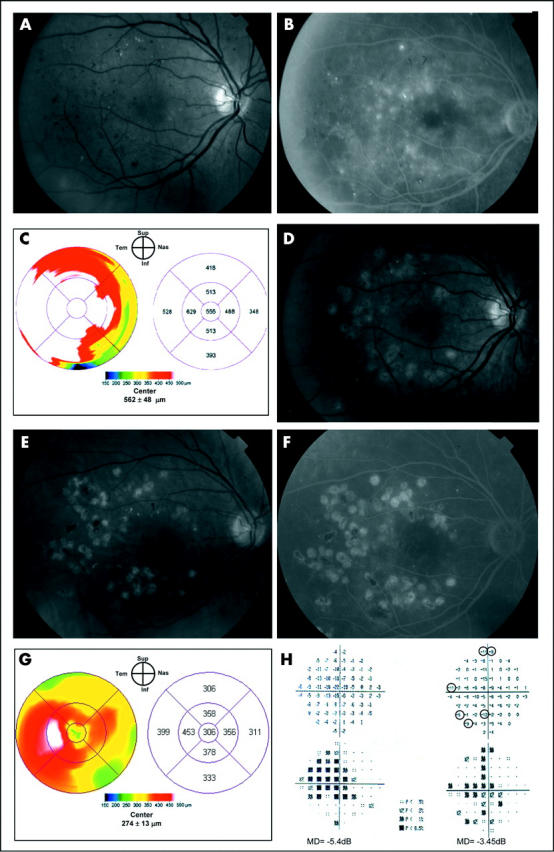
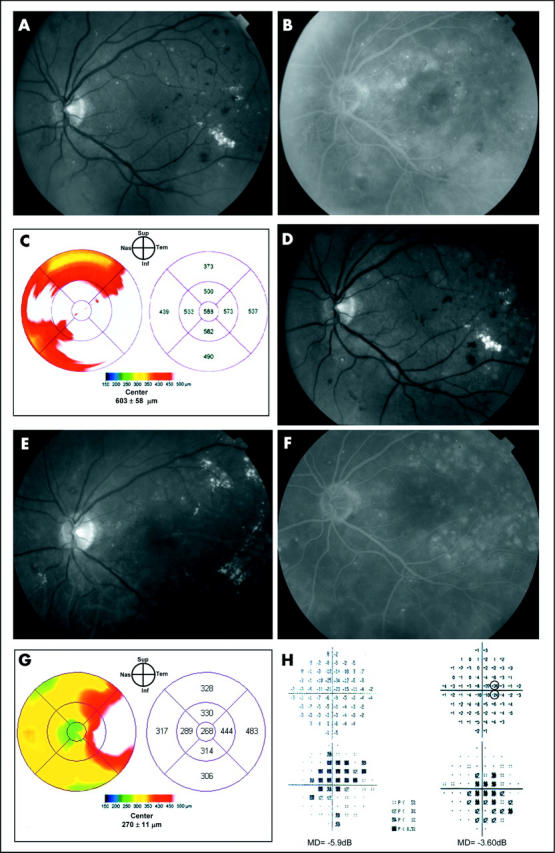
Methods: A prospective randomised pilot clinical trial in which 29 eyes of 24 diabetic patients with mild to moderate non-proliferative diabetic retinopathy (NPDR) and CSMO were randomised to either "classic" or "light" Nd:YAG 532 nm (frequency doubled) green laser. "Light" laser treatment differed from conventional ("classic") photocoagulation in that the energy employed was the lowest capable to produce barely visible burns at the level of the retinal pigment epithelium. Primary outcome measure was the change in foveal retinal thickness as measured by optical coherence tomography (OCT); secondary outcomes were the reduction/elimination of macular oedema on contact lens biomicroscopy and fluorescein angiography, change in visual acuity, contrast sensitivity, and mean deviation in the central 10 degrees visual field. Examiners were masked to patients' treatment.
Results: 14 eyes were assigned to "classic" and 15 were assigned to "light" laser treatment. At 12 months, seven (50%) of 14 eyes treated with "classic" and six (43%) of 14 eyes treated with "light" laser had a decrease of foveal retinal thickness on OCT (p = 0.79). A comparison of reduction/elimination of oedema, visual improvement, visual loss, change in contrast sensitivity, and mean deviation in the central 10 degrees showed no statistical difference between the groups at 12 months (p>0.05 for all groups).
Conclusions: This study suggests that "light" photocoagulation for CSMO may be as effective as "classic" laser treatment, thus supporting the rationale for a larger equivalence trial.
Figures
References
-
- Lee PP, Feldman ZW, Ostermann J, et al. Longitudinal prevalence of major eye diseases. Arch Ophthalmol 2003;121:1303–10. - PubMed
-
- Early Treatment Diabetic Retinopathy Study Research Group. Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study report number 1. Arch Ophthalmol 1985;103:1796–806. - PubMed
-
- Lee CM, Olk RJ. Modified grid laser photocoagulation for diffuse diabetic macular edema. Long-term visual results. Ophthalmology 1991;98:1594–602. - PubMed
-
- Akduman L, Olk RJ. Diode laser (810 nm) versus argon green (514 nm) modified grid photocoagulation for diffuse diabetic macular edema. Ophthalmology 1997;104:1433–41. - PubMed
-
- Striph GG, Hart WM Jr, Olk RJ. Modified grid laser photocoagulation for diabetic macular edema. The effect on the central visual field. Ophthalmology 1988;95:1673–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical