

Tumor vessel compression hinders perfusion of ultrasonographic contrast agents
- PMID: 15967105
- PMCID: PMC1501164
- DOI: 10.1593/neo.04730
Tumor vessel compression hinders perfusion of ultrasonographic contrast agents
Abstract
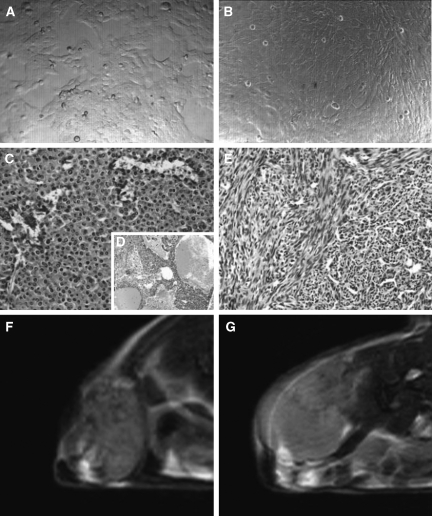
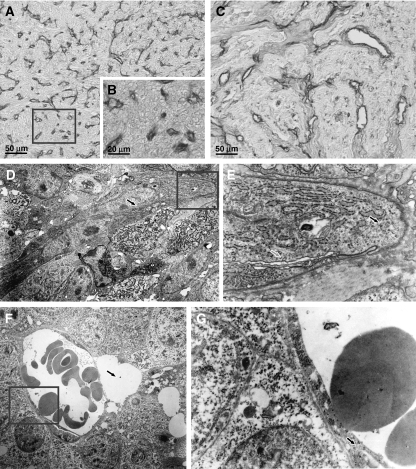
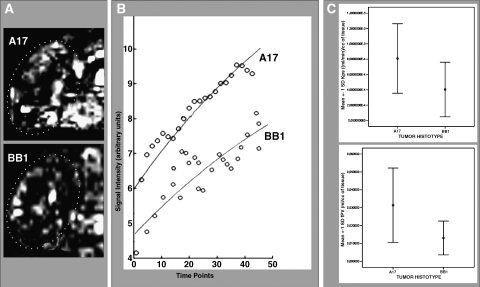
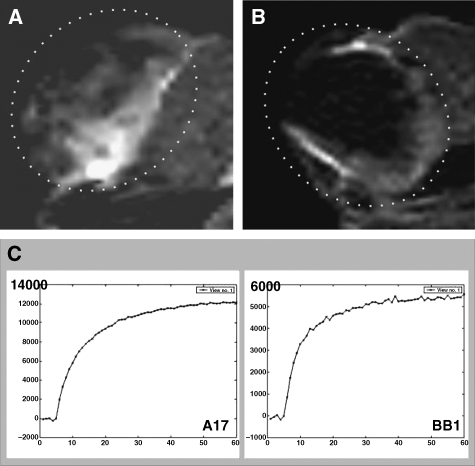
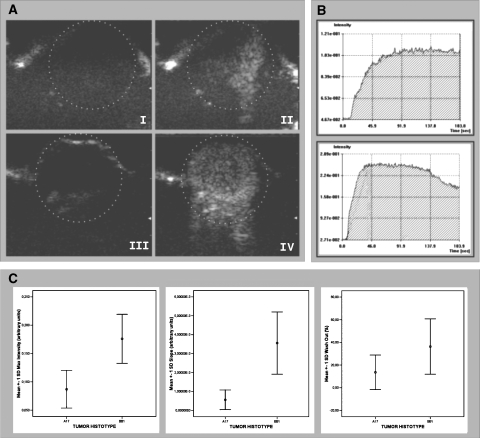
Contrast-enhanced ultrasound (CEUS) is an advanced approach to in vivo assessment of tumor vascularity and is being increasingly adopted in clinical oncology. It is based on 1- to 10 microm-sized gas microbubbles, which can cross the capillary beds of the lungs and are effective echo enhancers. It is known that high cell density, high transendothelial fluid exchange, and poorly functioning lymphatic circulation all provoke solid stress, which compresses vessels and drastically reduces tumor blood flow. Given their size, we supposed that the perfusion of microbubbles is affected by anatomic features of tumor vessels more than are contrast agents traditionally used in dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI). Here, we compared dynamic information obtained from CEUS and DCE-MRI on two experimental tumor models exhibiting notable differences in vessel anatomy. We found that tumors with small, flattened vessels show a much higher resistance to microbubble perfusion than to MRI contrast agents, and appear scarcely vascularized at CEUS examination, despite vessel volume adequate for normal function. Thus, whereas CEUS alone could induce incorrect diagnosis when tumors have small or collapsed vessels, integrated analysis using CEUS and DCE-MRI allows in vivo identification of tumors with a vascular profile frequently associated with malignant phenotypes.
Figures
References
-
- Kuhl CK, Mielcareck P, Klaschik S, Leutner C, Wardelmann E, Gieseke J, Schild HH. Dynamic breast MR imaging: are signal intensity time course data useful for differential diagnosis of enhancing lesions? Radiology. 1999;211:101–110. - PubMed
-
- Brasch RC, Li KC, Husband JE, Keogan MT, Neeman M, Padhani AR, Shames D, Turetschek K. In vivo monitoring of tumor angiogenesis with MR imaging. Acad Radiol. 2000;7:812–823. - PubMed
-
- Daldrup-Link HE, Brasch RC. Macromolecular contrast agents for MR mammography: current status. Eur Radiol. 2003;13:354–365. - PubMed
-
- Harvey CJ, Blomley MJ, Eckersley RJ, Cosgrove DO. Development in ultrasound contrast media. Eur Radiol. 2001;11:675–689. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources