

Repertoire, diversity, and differentiation of specific CD8 T cells are associated with immune protection against human cytomegalovirus disease
- PMID: 15967826
- PMCID: PMC2212029
- DOI: 10.1084/jem.20042408
Repertoire, diversity, and differentiation of specific CD8 T cells are associated with immune protection against human cytomegalovirus disease
Abstract
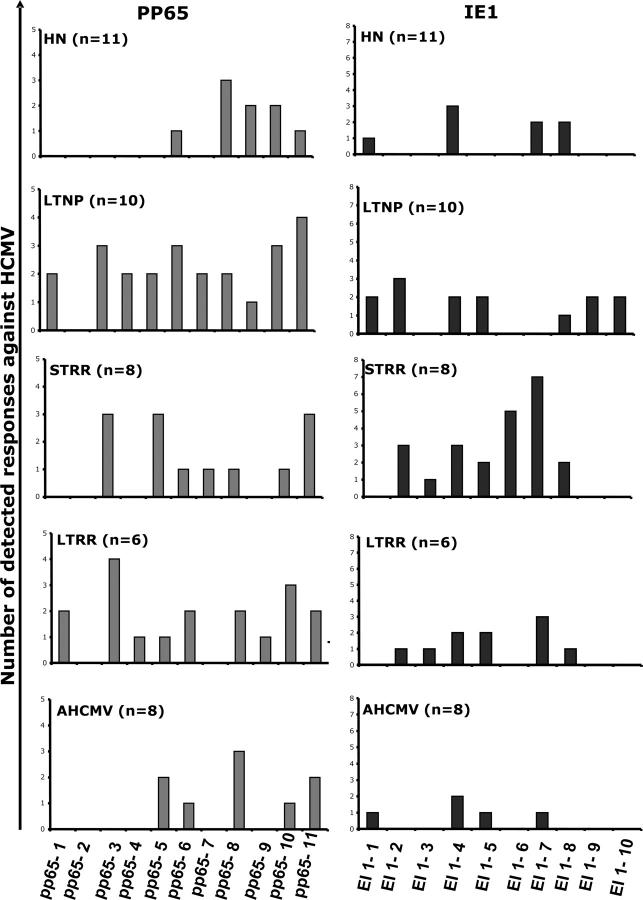
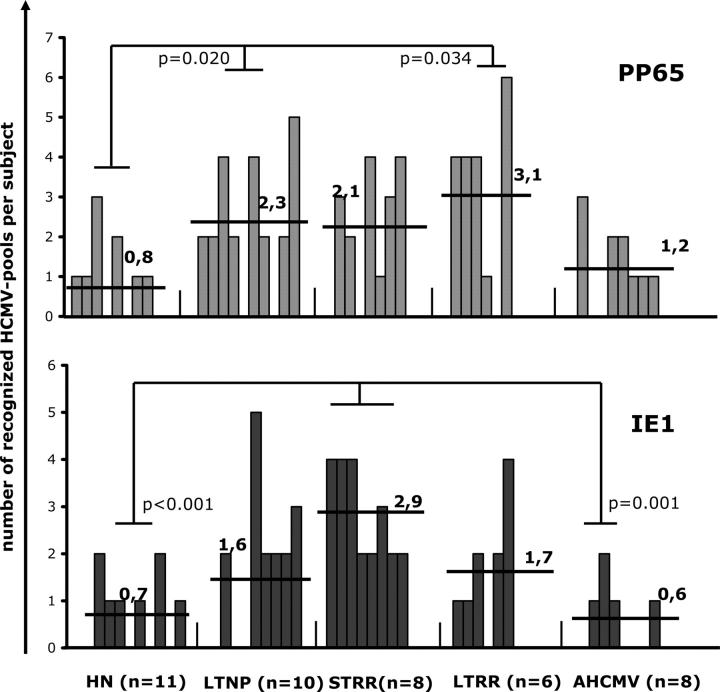
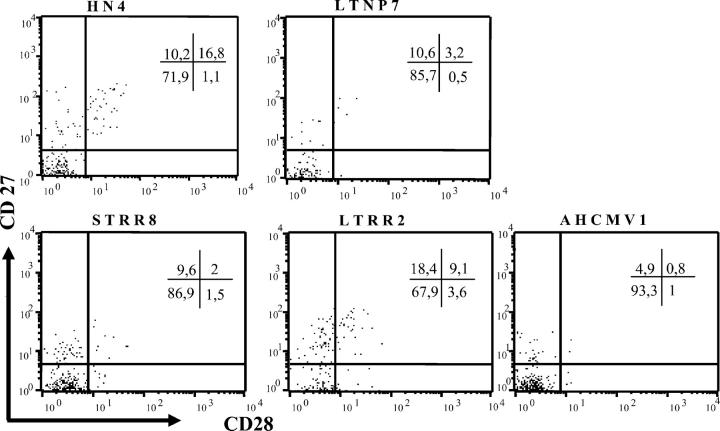
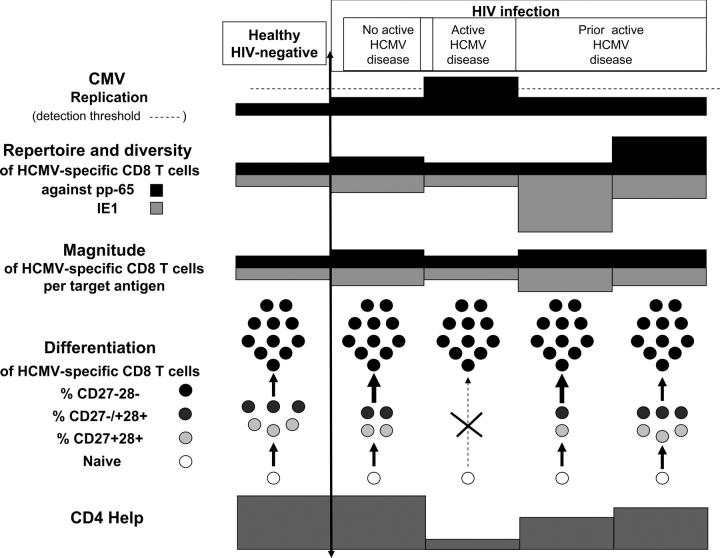
To determine the correlates of immune recovery from active human CMV (HCMV) disease, we compared the antigenic repertoire, diversity, magnitude, and differentiation of HCMV-specific CD8+ T cells in HIV-HCMV coinfected subjects with no, cured, or active HCMV disease and in healthy HIV-negative HCMV-positive controls. ELISPOT-IFN-gamma assays using peptide pools spanning the pp65 and immediate early 1 (IE1) HCMV proteins showed that HCMV-specific CD8+ T cells had a significantly broader antigenic repertoire and greater diversity in HIV-positive patients controlling HCMV replication than in those with active HCMV disease, but the magnitude of the CD8 T cell response did not differ between the different groups. HCMV-specific T cells mainly were focused against IE1 during the short-term recovery from retinitis, and switched toward pp65 during long-term recovery. HCMV-specific T cells displaying an "early" (CD8+CD27+CD28+) and "intermediate" (CD8+CD27-CD28+) differentiation phenotype were increased significantly during long-term recovery compared with other HIV-positive patients and were nearly undetectable during active HCMV disease. HCMV-specific T cells with a "late" (CD8+CD27-28-) differentiation phenotype predominated in all cases. Therefore, restoration of immune protection against HCMV after active HCMV disease in immunodeficient individuals is associated with enlarged repertoire and diversity, and with early differentiation of virus-specific CD8+ T cells, thus defining immune correlates of protection against diseases caused by persistent viruses.
Figures

References
-
- Mocarski, E.S., and C.T. Courcelle. 2001. Cytomegalovirus and their replication. Virology. 4th ed. B. Fields, D.M. Knipe, and P. Howley, editors. Raven Press, New York. 2626–2673.
-
- Pertel P., R. Hirschtick, J. Phair, J. Chmiel, L. Poggensee, and R. Murphy. 1992. Risk of developing cytomegalovirus retinitis in persons infected with the human immunodefiency virus. J. Acquir. Immune Defic. Synd. 5:1069–1074. - PubMed
-
- Gallant J.E., R.D. Moore, D.D. Richman, J. Keruly, and R.E. Chaisson. 1992. Incidence and natural history of cytomegalovirus disease in patients with advanced human immunodeficiency virus disease treated with zidovudine. J. Infect. Dis. 166:1223–1227. - PubMed
-
- Deayton J.R., A. Mocroft, P. Wilson, V.C. Emery, M.A. Johnson, and P.D. Griffiths. 1999. Changes in the natural history of cytomegalovirus retinitis following the introduction of highly active antiretroviral therapy. AIDS. 13:1203–1206. - PubMed
-
- O'Sullivan C.E., W.L. Drew, D.J. McMullen, R. Miner, J.Y. Lee, R.A. Kaslow, J.G. Lazar, and M.S. Saag. 1999. Decrease of cytomegalovirus replication in human immunodeficiency virus infected-patients after treatment with highly active antiretroviral therapy. J. Infect. Dis. 180:847–849. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
