

Subtle pleural metastasis without large effusion in lung cancer patients: preoperative detection on CT
- PMID: 15968148
- PMCID: PMC2686426
- DOI: 10.3348/kjr.2005.6.2.94
Subtle pleural metastasis without large effusion in lung cancer patients: preoperative detection on CT
Abstract
Objective: We wanted to describe the retrospective CT features of subtle pleural metastasis without large effusion that would suggest inoperable lung cancer.
Materials and methods: We enrolled 14 patients who had open thoracotomy attempted for lung cancer, but they were proven to be inoperable due to pleural metastasis. Our study also included 20 control patients who were proven as having no pleural metastasis. We retrospectively evaluated the nodularity and thickening of the pleura and the associated pleural effusion on the preoperative chest CT scans. We reviewed the histologic cancer types, the size, shape and location of the lung cancer and the associated mediastinal lymphadenopathy.
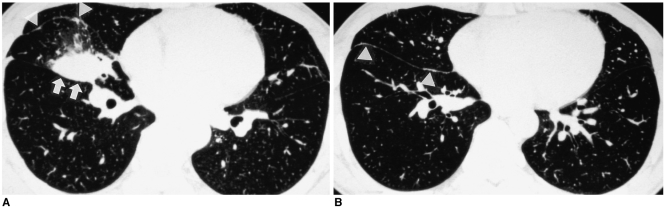
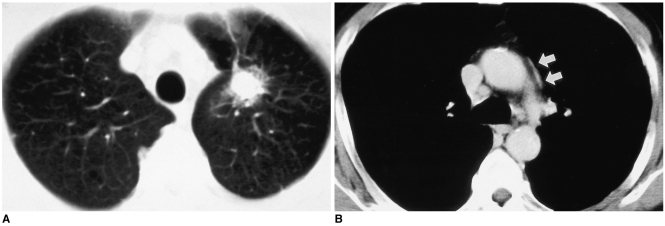
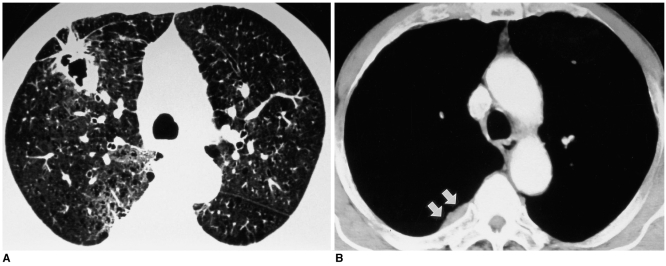
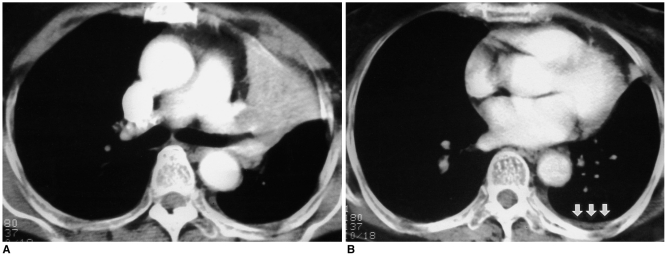
Results: Subtle pleural nodularity or focal thickening was noted in seven patients (50%) having pleural metastasis and also in three patients (15%) of control group who were without pleural metastasis. More than one of the pleural changes such as subtle pleural nodularity, focal thickening or effusion was identified in eight (57%) patients having pleural metastasis and also in three patients (15%) of the control group, and these findings were significantly less frequent in the control group patients than for the patients with pleural metastasis (p = 0.02). The histologic types of primary lung cancer in patients with pleural metastasis revealed as adenocarcinoma in 10 patients (71%) and squamous cell carcinoma in four patients (29%). The location, size and shape of the primary lung cancer and the associated mediastinal lymphadenopathy showed no significant correlation with pleural metastasis.
Conclusion: If any subtle pleural nodularity or thickening is found on preoperative chest CT scans of patients with lung cancer, the possibility of pleural metastasis should be considered.
Figures
References
-
- Kondo H, Asamura H, Suemasu K, Goya T, Tsuchiya R, Naruke T, et al. Prognostic significance of pleural lavage cytology immediately after thoracotomy in patients with lung cancer. J Thorac Cardiovasc Surg. 1993;106:1092–1097. - PubMed
-
- Kjellberg SI, Dresler CM, Goldberg M. Pleural cytologies in lung cancer without pleural effusions. Ann Thorac Surg. 1997;64:941–944. - PubMed
-
- Luh KT, Yang PC, Kuo SH, Chang DB, Yu CJ, Lee LN. Comparison of OK-432 and mitomycin C pleurodesis for malignant pleural effusion caused by lung cancer. A randomized trial. Cancer. 1992;69:674–679. - PubMed
-
- Martini N, Bains MS, Beattie EJ., Jr Indications for pleurectomy in malignant effusion. Cancer. 1975;35:734–738. - PubMed
-
- Moffett MJ, Ruckdeschel JC. Bleomycin and tetracycline in malignant pleural effusions: a review. Semin Oncol. 1992;19:59–63. - PubMed
