

Laparoscopic Roux-en-Y versus mini-gastric bypass for the treatment of morbid obesity: a prospective randomized controlled clinical trial
- PMID: 15973097
- PMCID: PMC1357700
- DOI: 10.1097/01.sla.0000167762.46568.98
Laparoscopic Roux-en-Y versus mini-gastric bypass for the treatment of morbid obesity: a prospective randomized controlled clinical trial
Abstract
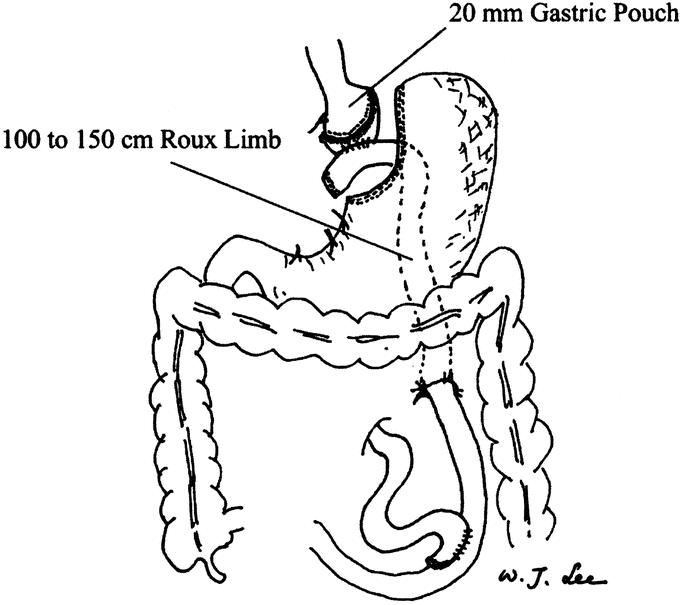
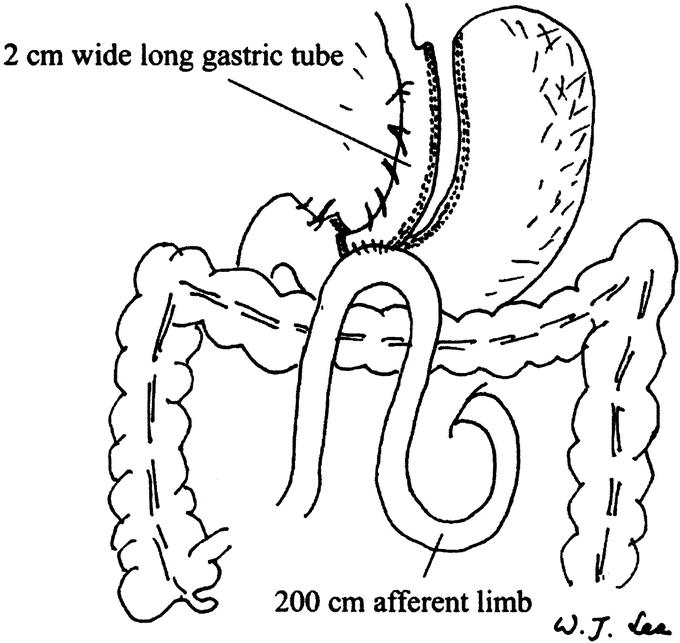
Objectives: This prospective, randomized trial compared the safety and effectiveness of laparoscopic Roux-en-Y gastric bypass (LRYGBP) and laparoscopic mini-gastric bypass (LMGBP) in the treatment of morbid obesity.
Summary background data: LRYGBP has been the gold standard for the treatment of morbid obesity. While LMGBP has been reported to be a simple and effective treatment, data from a randomized trial are lacking.
Methods: Eighty patients who met the NIH criteria were recruited and randomized to receive either LRYGBP (n = 40) or LMGBP (n = 40). The minimum postoperative follow-up was 2 years (mean, 31.3 months). Perioperative data were assessed. Late complication, excess weight loss, BMI, quality of life, and comorbidities were determined. Changes in quality of life were assessed using the Gastro-Intestinal Quality of Life Index (GIQLI).
Results: There was one conversion (2.5%) in the LRYGBP group. Operation time was shorter in LMGBP group (205 versus 148, P < 0.05). There was no mortality in each group. The operative morbidity rate was higher in the LRYGBP group (20% versus 7.5%, P < 0.05). The late complications rate was the same in the 2 groups (7.5%) with no reoperation. The percentage of excess weight loss was 58.7% and 60.0% at 1 and 2 years, respectively, in the LPYGBP group, and 64.9% and 64.4% in the LMGBP group. The residual excess weight <50% at 2 years postoperatively was achieved in 75% of patients in the LRYGBP group and 95% in the LMGBP group (P < 0.05). A significant improvement of obesity-related clinical parameters and complete resolution of metabolic syndrome in both groups were noted. Both gastrointestinal quality of life increased significantly without any significant difference between the groups.
Conclusion: Both LRYGBP and LMGBP are effective for morbid obesity with similar results for resolution of metabolic syndrome and improvement of quality of life. LMGBP is a simpler and safer procedure that has no disadvantage compared with LRYGBP at 2 years of follow-up.
Figures
Comment in
-
Is laparoscopic Roux-en-Y gastric bypass superior to mini-gastric bypass for the treatment of morbid obesity?Nat Clin Pract Gastroenterol Hepatol. 2006 Jan;3(1):16-7. doi: 10.1038/ncpgasthep0391. Nat Clin Pract Gastroenterol Hepatol. 2006. PMID: 16397605 No abstract available.
References
-
- Must A, Spadano J, Coakley EH, et al. The disease burden associated with overweight and obesity. JAMA. 1999;282:1523–1529. - PubMed
-
- Fontaine KR, Redden DT, Wang C, et al. Years of life lost due to obesity. JAMA. 2003;289:187–193. - PubMed
-
- NIH Conference: Gastrointestinal surgery for severe obesity. Ann Intern Med. 1991;115:959–961. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
