

Evaluation of the learning curve in laparoscopic colorectal surgery: comparison of right-sided and left-sided resections
- PMID: 15973105
- PMCID: PMC1357708
- DOI: 10.1097/01.sla.0000167857.14690.68
Evaluation of the learning curve in laparoscopic colorectal surgery: comparison of right-sided and left-sided resections
Abstract
Objective: To provide a multidimensional analysis of the learning curve in major laparoscopic colonic and rectal surgery and compare outcomes between right-sided versus left-sided resections.
Summary background data: The laparoscopic learning curve is known to vary between surgeons, may be influenced by the patient selection and operative complexity, and requires appropriate case-mix adjustment.
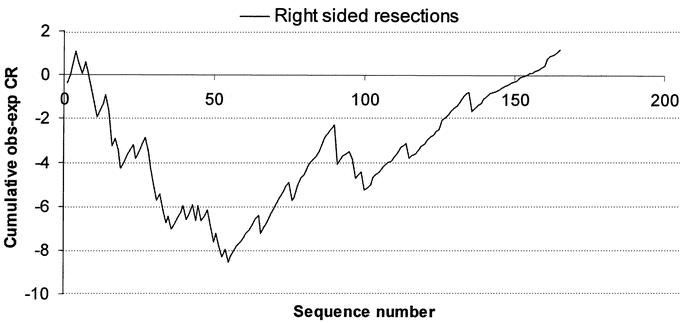
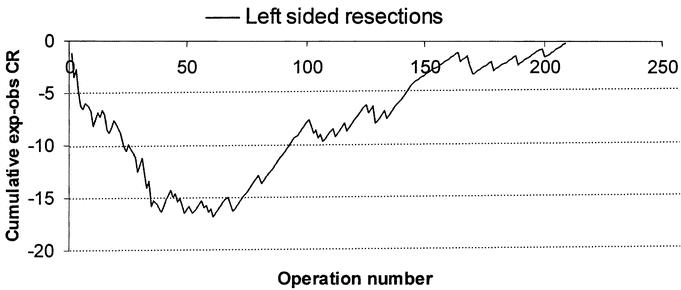
Methods: This is a descriptive single-center study using routinely collected clinical data from 900 patients undergoing laparoscopic surgery between November 1991 and April 2003. Outcome measures included operation time, conversion rate (CR), and readmission and postoperative complication rates. Multifactorial logistic regression analysis was used to identify patient-, surgeon-, and procedure-related factors associated with conversion of laparoscopic to open surgery. A risk-adjusted Cumulative Sum (CUSUM) model was used for evaluating the learning curve for right and left-sided resections.
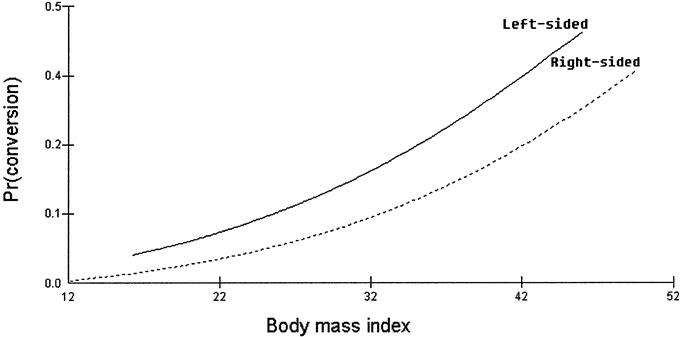
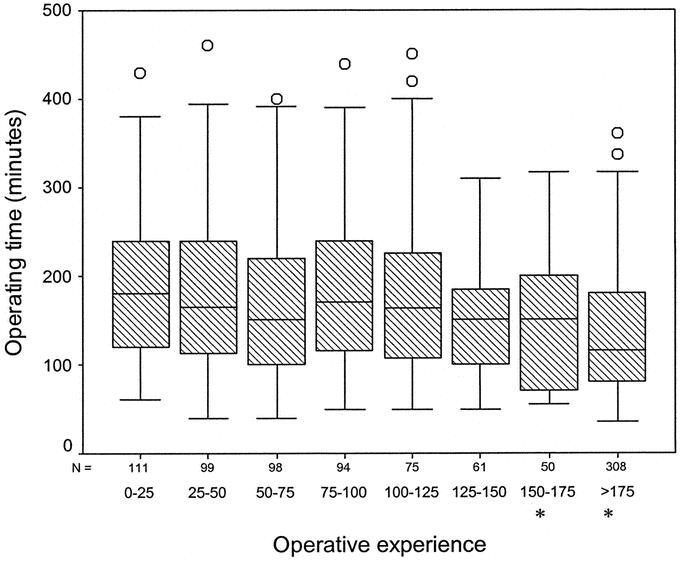
Results: The conversion rate for right-sided colonic resections was 8.1% (n = 457) compared with 15.3% for left-sided colorectal resections (n = 443). Independent predictors of conversion of laparoscopic to open surgery were the body mass index (BMI) (odds ratio [OR] = 1.07 per unit increase), ASA grade (OR = 1.63 per unit increase), type of resection (left colorectal versus right colonic procedures, OR = 1.5), presence of intra-abdominal abscess (OR = 5.0) or enteric fistula (OR = 4.6), and surgeon's experience (OR 0.9 per 10 additional cases performed). Having adjusted for case-mix, the CUSUM analysis demonstrated a learning curve of 55 cases for right-sided colonic resections versus 62 cases for left-sided resections. Median operative time declined with operative experience (P<0.001). Readmission rates and postoperative complications remained unchanged throughout the series and were not dependent on operative experience.
Conclusions: Conversion rates for laparoscopic colectomy are dependent on a multitude of factors that require appropriate adjustment including the learning curve (operative experience) for individual surgeons. The laparoscopic model described can be used as the basis for performance monitoring between or within institutions.
Figures
References
-
- Senagore AJ, Duepree HJ, Delaney CP, et al. Cost structure of laparoscopic and open sigmoid colectomy for diverticular disease: similarities and differences. Dis Colon Rectum. 2002;45:485–490. - PubMed
-
- Schlachta CM, Mamazza J, Seshadri PA, et al. Defining a learning curve for laparoscopic colorectal resections. Dis Colon Rectum. 2001;44:217–222. - PubMed
-
- Ramsay CR, Wallace SA, Garthwaite PH, et al. Assessing the learning curve effect in health technologies: lessons from the nonclinical literature. Int J Technol Assess Health Care. 2002;18:1–10. - PubMed
-
- Ramsay CR, Grant AM, Wallace SA, et al. Statistical assessment of the learning curves of health technologies. Health Technol Assess. 2001;5:1–79. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
