

Clinicopathologic analysis of early ampullary cancers with a focus on the feasibility of ampullectomy
- PMID: 15973106
- PMCID: PMC1357709
- DOI: 10.1097/01.sla.0000167853.04171.bb
Clinicopathologic analysis of early ampullary cancers with a focus on the feasibility of ampullectomy
Abstract
Objective: The purpose of this study was to evaluate whether ampullectomy can substitute for pancreatoduodenectomy (PD) in early ampullary cancer by clinicopathologic study.
Summary background data: Although ampullectomy has been attempted in early ampullary cancer (pTis, pT1), the indication and extent of resection have not been established.
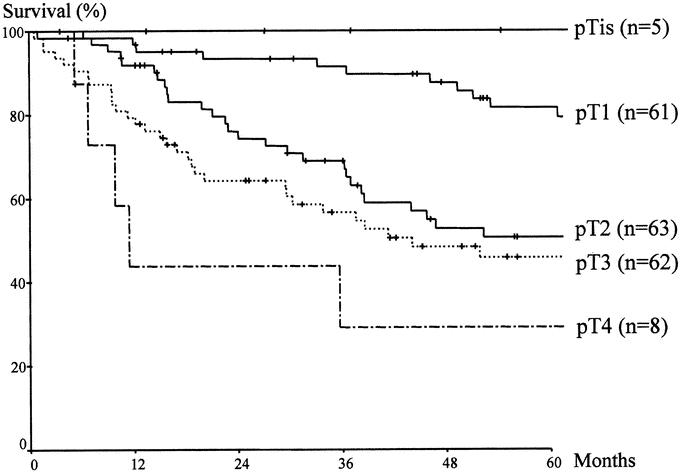
Methods: Of 201 patients who had undergone PD for ampullary cancer between 1986 and 2002, 67 patients with a histologic diagnosis of pTis (n = 5) or pT1 (n = 62) cancer were analyzed retrospectively. Pathologic PD specimens were reviewed to analyze the cancer spread pattern, and medical records were reviewed for clinical outcomes.
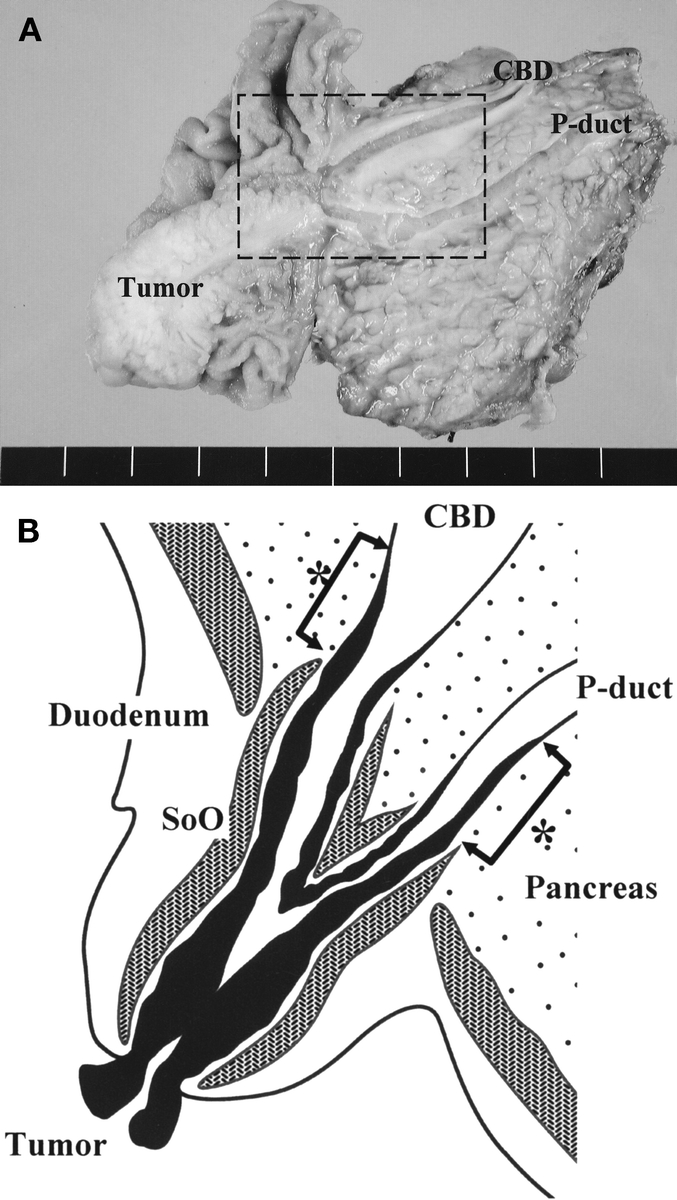
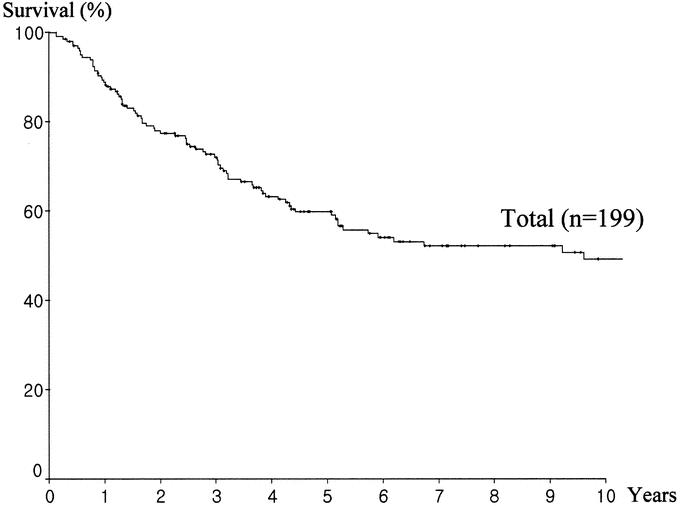
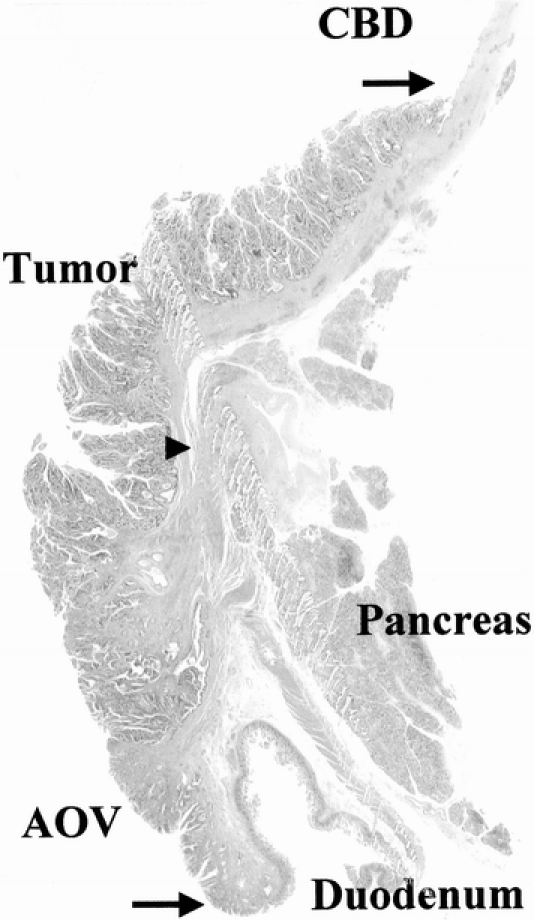
Results: The 5-year survival rate of the 66 patients with early ampullary cancer (excluding one mortality) was 83.7%. Recurrence was confirmed in 12 patients (18.2%) and all died because of the recurrence. Pathologic review showed that 22 patients (32.8%) had at least one risk factor for failure after ampullectomy: lymph node metastasis (n = 6, 9.0%), perineural invasion (n = 1), or mucosal tumor infiltration along the CBD or P-duct (n = 15, 22.4%). Mean lengths of invasion into the CBD or the P-duct beyond the sphincter of Oddi were 7.7 mm (range, 1-25 mm) or 6.3 mm (range, 2-18 mm), respectively. Moreover, these risk factors were not correlated with tumor size, histologic grade, or the gross morphology of the primary tumor, although pTis cancer or pT1 cancer sized 1.0 cm or less was found to be least associated with risk factors.
Conclusions: Ampullectomy for early ampullary cancer should not be considered an alternative operation to PD because of the high possibility of recurrence. PD should be preferably performed for adequate radical resection, even in early ampullary cancer, and ampullectomy should be reserved for those who have pTis or pT1 cancer sized 1.0 cm or less with high operative risk.
Figures
Similar articles
-
Long-term prognosis of surgical treatment for early ampullary cancers and implications for local ampullectomy.BMC Surg. 2015 Mar 22;15:32. doi: 10.1186/s12893-015-0019-z. BMC Surg. 2015. PMID: 25888004 Free PMC article.
-
Transduodenal ampullectomy provides a less invasive technique to cure early ampullary cancer.BMC Surg. 2016 Jun 1;16(1):36. doi: 10.1186/s12893-016-0156-z. BMC Surg. 2016. PMID: 27251044 Free PMC article.
-
What is an adequate surgical management for pTis and pT1 early ampullary carcinoma?Hepatogastroenterology. 2014 Jan-Feb;61(129):12-7. Hepatogastroenterology. 2014. PMID: 24895785
-
Experience with 647 consecutive tumors of the duodenum, ampulla, head of the pancreas, and distal common bile duct.Ann Surg. 1989 Oct;210(4):544-54; discussion 554-6. doi: 10.1097/00000658-198910000-00015. Ann Surg. 1989. PMID: 2679459 Free PMC article. Review.
-
Is local excision of pT1-ampullary carcinomas justified?Eur J Surg Oncol. 1996 Aug;22(4):366-71. doi: 10.1016/s0748-7983(96)90286-3. Eur J Surg Oncol. 1996. PMID: 8783654 Review.
Cited by
-
Investigation of the Indications for Endoscopic Papillectomy and Transduodenal Ampullectomy for Ampullary Tumors.J Clin Med. 2021 Sep 28;10(19):4463. doi: 10.3390/jcm10194463. J Clin Med. 2021. PMID: 34640487 Free PMC article.
-
Prognostic factors of carcinoma of the ampulla of Vater after surgery.Tumour Biol. 2014 Feb;35(2):1143-8. doi: 10.1007/s13277-013-1153-9. Epub 2013 Sep 12. Tumour Biol. 2014. PMID: 24026886
-
Trends in incidence and management of cancer of the ampulla of Vater.World J Gastroenterol. 2014 Aug 7;20(29):10144-50. doi: 10.3748/wjg.v20.i29.10144. World J Gastroenterol. 2014. PMID: 25110442 Free PMC article.
-
Histopathologic differentiation as a prognostic factor in patients with carcinoma of the hepatopancreatic ampulla of Vater.J Int Med Res. 2018 Nov;46(11):4634-4639. doi: 10.1177/0300060518786920. Epub 2018 Jul 20. J Int Med Res. 2018. PMID: 30027790 Free PMC article.
-
Carcinoma of the papilla of Vater: are endoscopic appearance and endoscopic biopsy discordant?J Gastrointest Surg. 2006 Sep-Oct;10(8):1140-3. doi: 10.1016/j.gassur.2006.05.005. J Gastrointest Surg. 2006. PMID: 16966033
References
-
- Monson JRT, Donohue JH, McEntee GP, et al. Radical resection for carcinoma of the ampulla of Vater. Arch Surg. 1991;126:353–357. - PubMed
-
- Allema JH, Reinders ME, van Gulik TM, et al. Results of pancreaticoduodenectomy for ampullary carcinoma and analysis of prognostic factors for survival. Surgery. 1995;117:247–253. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
