

Clustered local transmission and asymptomatic Plasmodium falciparum and Plasmodium vivax malaria infections in a recently emerged, hypoendemic Peruvian Amazon community
- PMID: 15975146
- PMCID: PMC1190209
- DOI: 10.1186/1475-2875-4-27
Clustered local transmission and asymptomatic Plasmodium falciparum and Plasmodium vivax malaria infections in a recently emerged, hypoendemic Peruvian Amazon community
Abstract
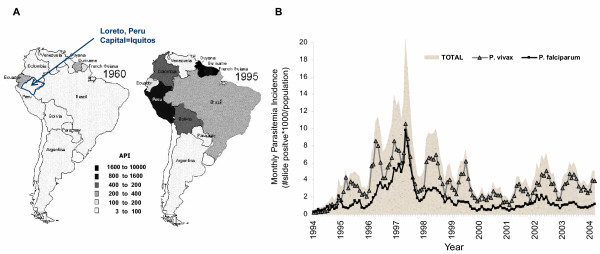
Background: There is a low incidence of malaria in Iquitos, Peru, suburbs detected by passive case-detection. This low incidence might be attributable to infections clustered in some households/regions and/or undetected asymptomatic infections.
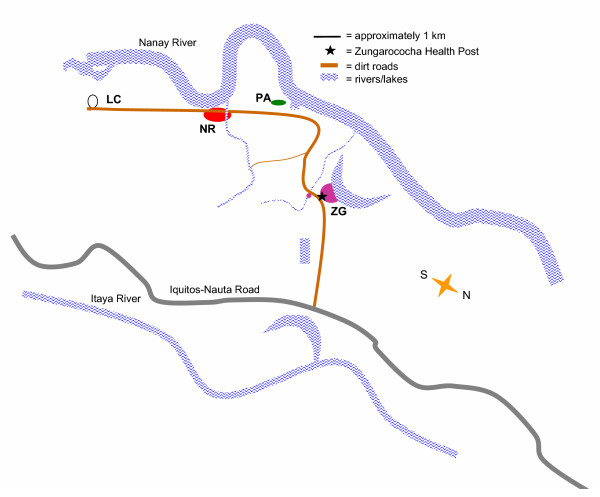
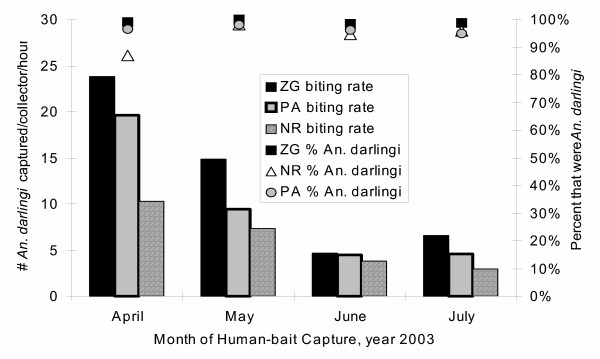
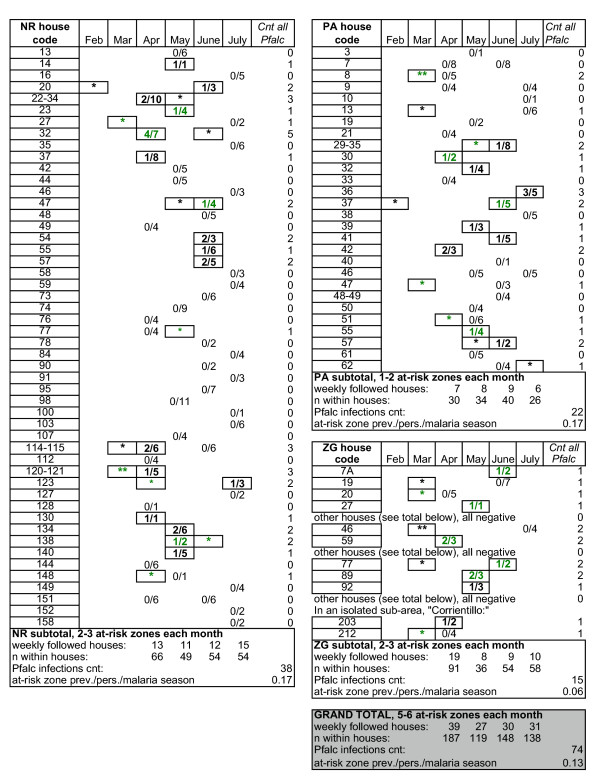
Methods: Passive case-detection (PCD) during the malaria season (February-July) and an active case-detection (ACD) community-wide survey (March) surveyed 1,907 persons. Each month, April-July, 100-metre at-risk zones were defined by location of Plasmodium falciparum infections in the previous month. Longitudinal ACD and PCD (ACP+PCD) occurred within at-risk zones, where 137 houses (573 persons) were randomly selected as sentinels, each with one month of weekly active sampling. Entomological captures were conducted in the sentinel houses.
Results: The PCD incidence was 0.03 P. falciparum and 0.22 Plasmodium vivax infections/person/malaria-season. However, the ACD+PCD prevalence was 0.13 and 0.39, respectively. One explanation for this 4.33 and 1.77-fold increase, respectively, was infection clustering within at-risk zones and contiguous households. Clustering makes PCD, generalized to the entire population, artificially low. Another attributable-factor was that only 41% and 24% of the P. falciparum and P. vivax infections were associated with fever and 80% of the asymptomatic infections had low-density or absent parasitaemias the following week. After accounting for asymptomatic infections, a 2.6-fold increase in ACD+PCD versus PCD was attributable to clustered transmission in at-risk zones.
Conclusion: Even in low transmission, there are frequent highly-clustered asymptomatic infections, making PCD an inadequate measure of incidence. These findings support a strategy of concentrating ACD and insecticide campaigns in houses adjacent to houses were malaria was detected one month prior.
Figures
References
-
- Manguin S, Roberts DR, Peyton EL, Fernandez-Salas I, Barreto M, Fernandez Loayza R, Elgueta Spinola R, Martinez Granaou R, Rodriguez MH. Biochemical systematics and population genetic structure of Anopheles pseudopunctipennis, vector of malaria in Central and South America. Am J Trop Med Hyg. 1995;53:362–377. - PubMed
-
- Arata AA, Ruebush TK, Porter CH, Stein JD, Lounibos LP, Fernandez DM. Malaria in the Peruvian Amazon: a review of the epidemiology, entomology and insecticide resistance of vectors. In: 60 ARN, editor. Environmental Health Project. Washington, DC: USAID; 1999.
-
- Snow RW, Omumbo JA, Lowe B, Molyneux CS, Obiero JO, Palmer A, Weber MW, Pinder M, Nahlen B, Obonyo C, Newbold C, Gupta S, Marsh K. Relation between severe malaria morbidity in children and level of Plasmodium falciparum transmission in Africa [see comments] Lancet. 1997;349:1650–1654. doi: 10.1016/S0140-6736(97)02038-2. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
