

Bone mineral density, body mass index and cigarette smoking among Iranian women: implications for prevention
- PMID: 15975151
- PMCID: PMC1184084
- DOI: 10.1186/1471-2474-6-34
Bone mineral density, body mass index and cigarette smoking among Iranian women: implications for prevention
Abstract
Background: While risk factors of osteoporosis in Western populations have been extensively documented, such a profile has not been well studied in Caucasians of non-European origin. This study was designed to estimate the modifiable distribution and determinants of bone mineral density (BMD) among Iranian women in Australia.
Methods: Ninety women aged 35 years and older completed a questionnaire on socio-demographic and lifestyle factors. BMD was measured at the lumbar spine (LS) and femoral neck (FN) using DXA (GE Lunar, WI, USA), and was expressed in g/cm2 as well as T-score.
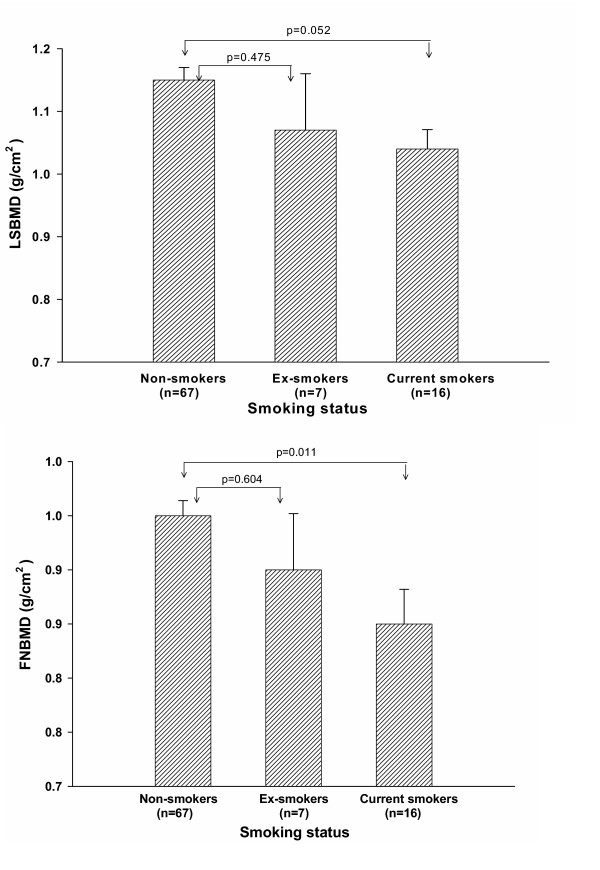
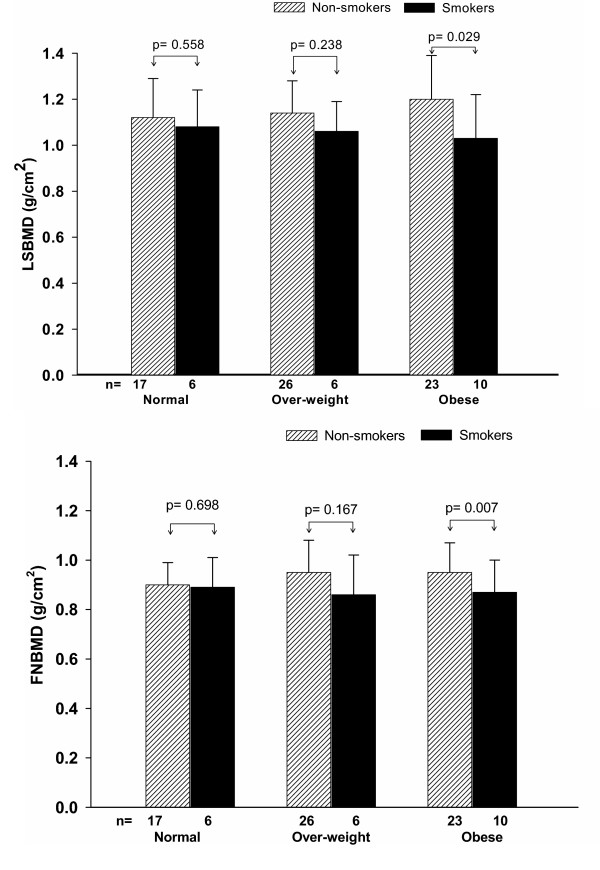
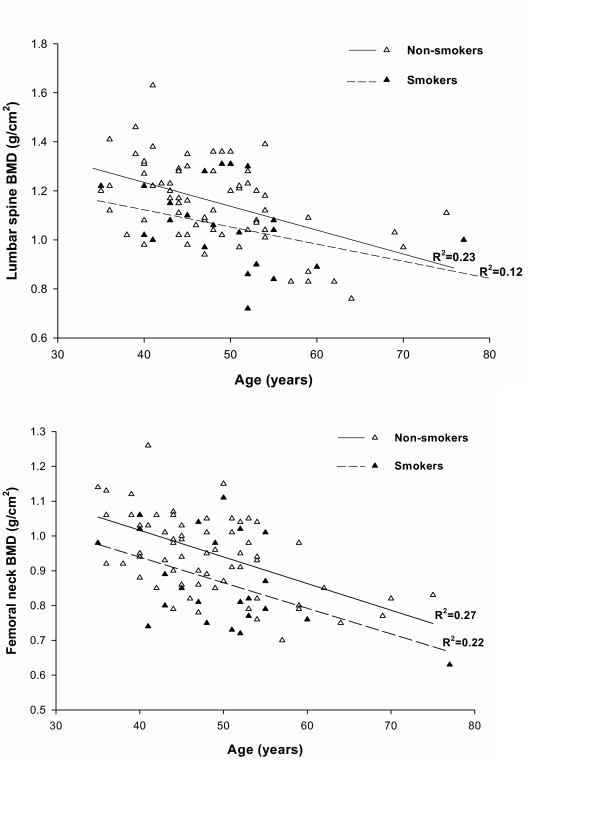
Results: In multiple regression analysis, advancing age, lower body mass index (BMI), and smoking were independently associated with LS and FN BMD, with the 3 factors collectively accounting for 30% and 38% variance of LS and FN BMD, respectively. LS and FN BMD in smokers was 8% lower than that in non-smokers. Further analysis of interaction between BMI and smoking revealed that the effect of smoking was only observed in the obese group (p = 0.029 for LSBMD and p = 0.007 for FNBMD), but not in the overweight and normal groups. Using T-scores from two bone sites the prevalence of osteoporosis (T-scores <or= -2.5) was 3.8% and 26.3% in pre-and post-menopausal women, respectively. Among current smokers, the prevalence was higher (31.3%) than that among ex-smokers (28.6%) and non-smokers (7.5%).
Conclusion: These data, for the first time, indicate that apart from advancing age and lower body mass index, cigarette smoking is an important modifiable determinant of bone mineral density in these Caucasians of non-European origin.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
