

The use of LYVE-1 antibody for detecting lymphatic involvement in patients with malignant melanoma of known sentinel node status
- PMID: 15976338
- PMCID: PMC1770724
- DOI: 10.1136/jcp.2004.020123
The use of LYVE-1 antibody for detecting lymphatic involvement in patients with malignant melanoma of known sentinel node status
Abstract
Background: Sentinel node (SN) status is the most important prognostic indicator in patients with cutaneous melanoma without clinically evident metastatic spread, but the procedure is associated with considerable morbidity. The LYVE-1 lymphatic marker offers the possibility of studying lymphangiogenesis and tumour metastasis within the primary excision.
Aims: To establish whether lymphatic vessel numbers/distribution within the primary tumour correlated with SN status. To assess whether tumour cells were easily demonstrable within lymphatics and could be used as a surrogate for SN status.
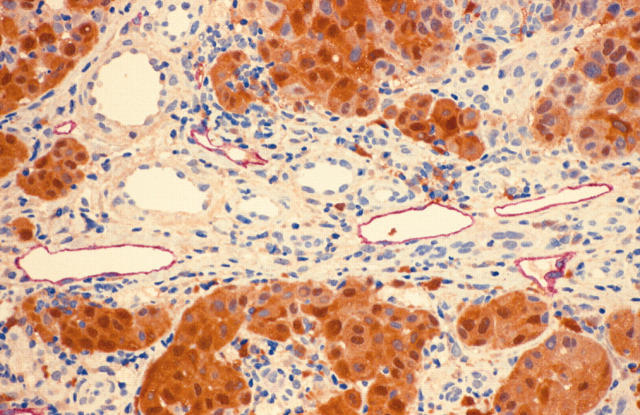
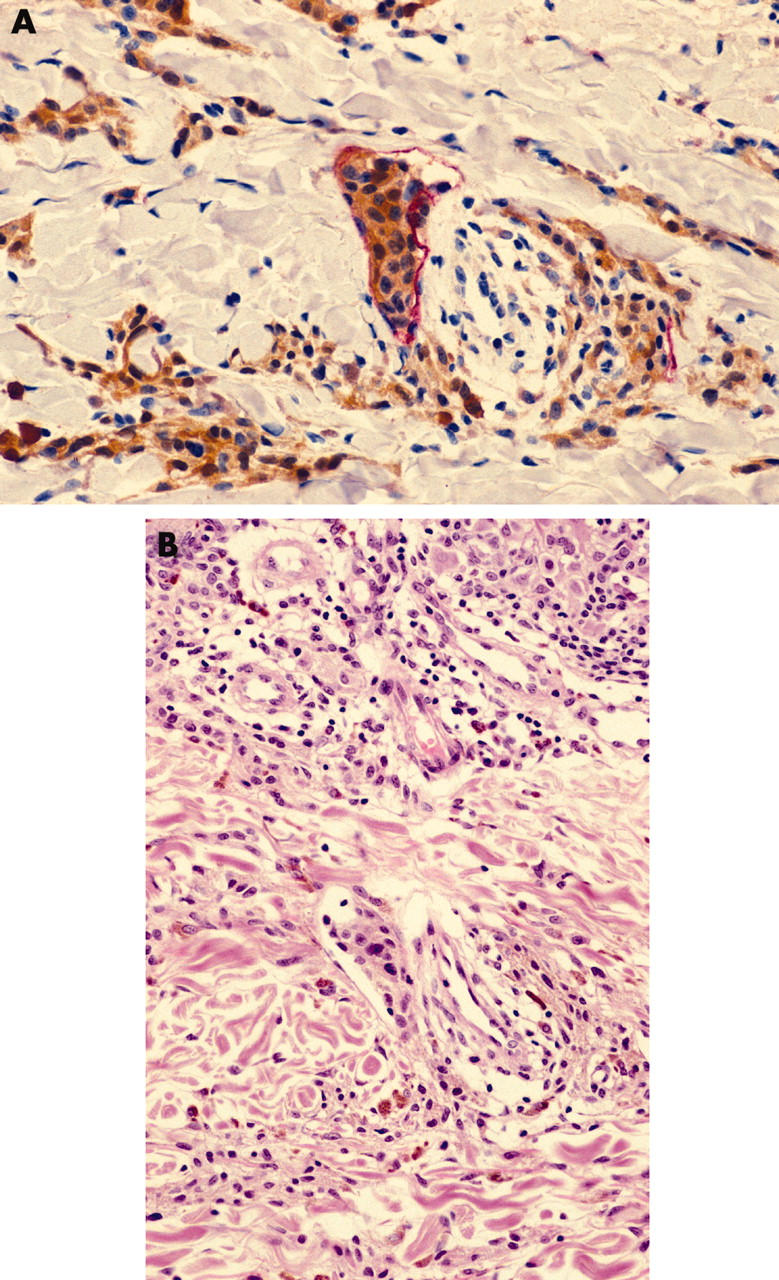
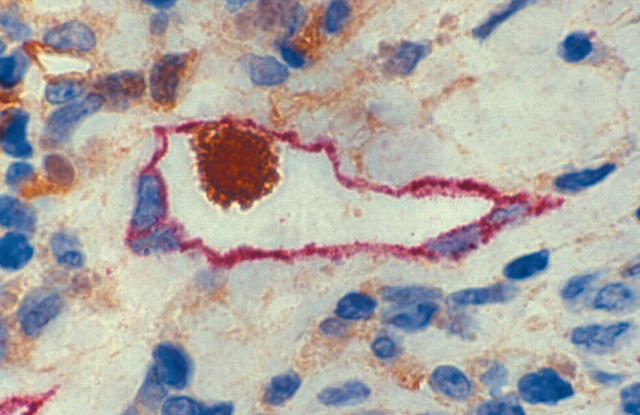
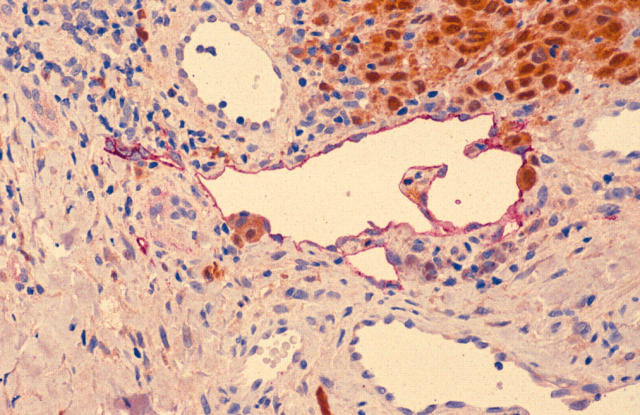
Methods: Double immunostaining for LYVE-1 and S100 in cutaneous biopsies from 18 SN+ patients with no lymphatic/vascular involvement on routine histology and 18 SN- patients matched for tumour thickness and ulceration.
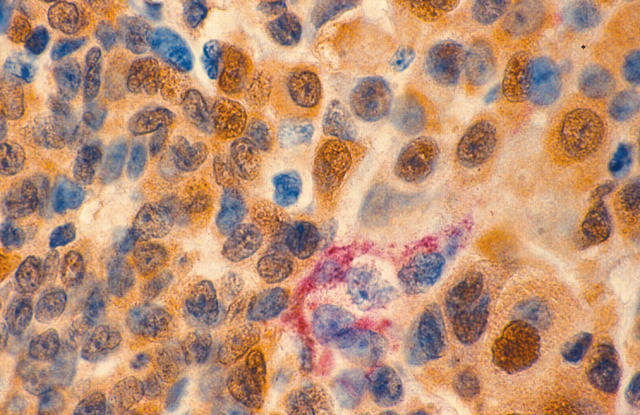
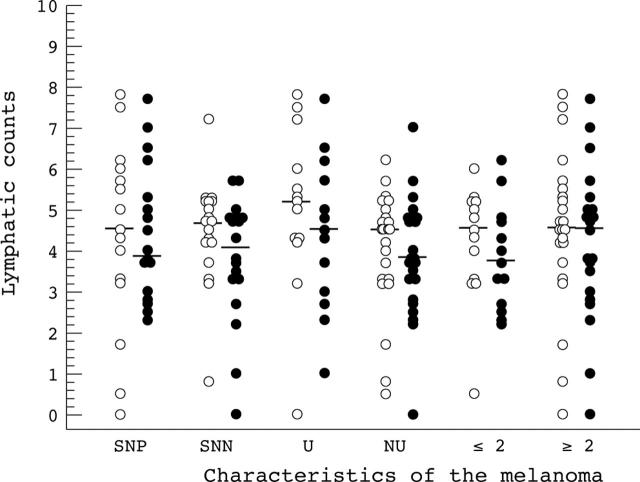
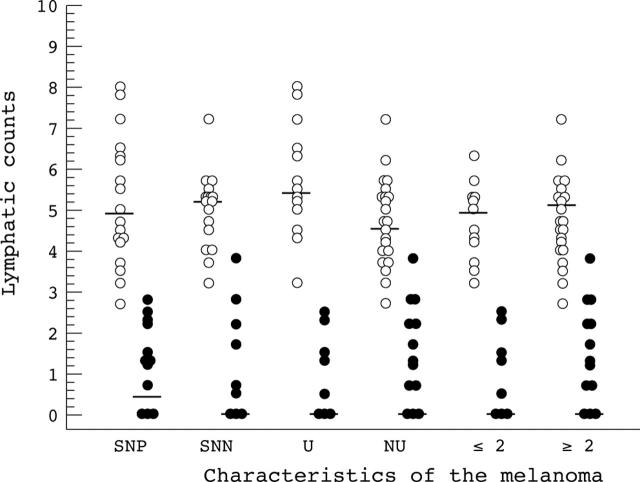
Results: Lymphatic vessels were detected in all cases. Vessels within the tumour mass were suggestive of active lymphangiogenesis; those outside were mainly mature vessels with well defined walls. Tumour cells within lymphatics were detected in one of 18 SN- and five of 18 SN+ patients. Lymphatics containing tumour cells were all outside the tumour mass in well formed vessels, suggesting melanoma cell invasion into preformed lymphatics. There was no significant difference in lymphatic counts between SN+ and SN- patients. Although peritumorous lymphatic counts were higher in ulcerated than non-ulcerated melanomas, they did not vary with Breslow thickness.
Conclusion: LYVE-1 staining can reliably demonstrate lymphatic vessel distribution, but lymphatic counts cannot predict melanoma metastatic potential and cannot substitute for SN biopsy. LYVE-1 immunostaining can detect melanoma cells within lymphatics, but is unreliable in predicting melanoma metastasis, failing to detect metastatic spread in more than two thirds of patients with regional node metastasis.
Figures

References
-
- Gerschenwald J, Thompson W, Mansfield P, et al. Multi-institutional melanoma lymphatic mapping experience: the prognostic value of sentinel node status in 612 stage I and II melanoma patients. J Clin Oncol 1999;3:976–83. - PubMed
-
- Wagner J, Corbett L, Myung Park H, et al. Sentinel lymph node biopsy for melanoma. Experience with 234 consecutive procedures. Plast Reconst Surg 2000;105:1956–66. - PubMed
-
- Landi G, Polverelli M, Moscatelli G, et al. Sentinel lymph node biopsy in patients with primary cutaneous melanoma; study of 455 cases. J Eur Acad Dermatol Venereol 2000;14:35–45. - PubMed
-
- Shivers S, Xang X, Li W, et al. Molecular staging of malignant melanoma. JAMA 1998;280:1410–15. - PubMed
-
- Blaheta H-J, Ellwanger U, Schittek B, et al. Examination of regional lymph nodes by sentinel node biopsy and molecular analysis provides new staging facilities in primary cutaneous melanoma. J Invest Dermatol 2000;14:637–42. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous