

Use of native or platelet count adjusted platelet rich plasma for platelet aggregation measurements
- PMID: 15976345
- PMCID: PMC1770722
- DOI: 10.1136/jcp.2004.022129
Use of native or platelet count adjusted platelet rich plasma for platelet aggregation measurements
Abstract
Background: It is still not clear whether native or platelet count adjusted platelet rich plasma (PRP) should be used for platelet aggregation measurements.
Aim: To evaluate the necessity of using adjusted PRP in platelet function testing.
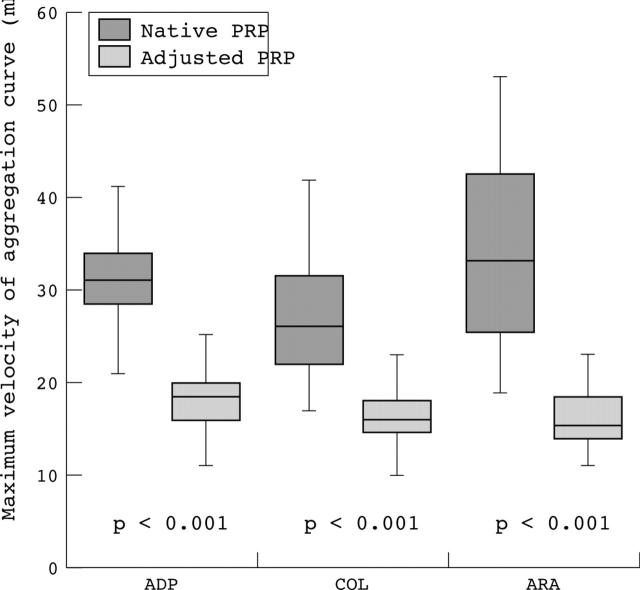
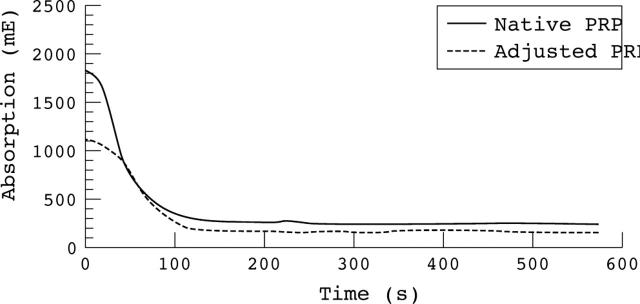
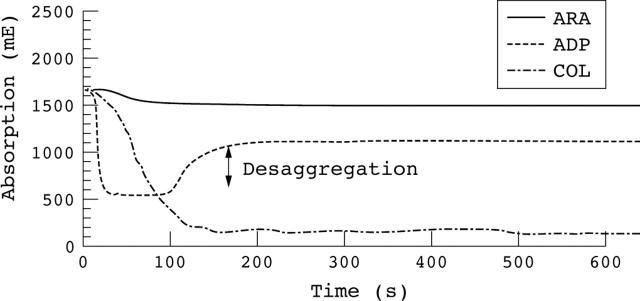
Methods: Platelet aggregation with native PRP and adjusted PRP (platelet count: 250/nl, obtained by diluting native PRP with platelet poor plasma) was performed on the Behring Coagulation Timer (BCT(R)) using ADP, collagen, and arachidonic acid as agonists. Healthy subjects, patients on antiplatelet treatment, and patients with thrombocytosis (platelet counts in PRP > 1250/nl) were investigated.
Results: No significant differences in the maximum aggregation response were seen when using either native or adjusted PRP from healthy subjects and patients on antiplatelet treatment. Nevertheless, some patients taking aspirin or clopidogrel showed reduced inhibition of ADP and arachidonic acid induced aggregation in adjusted PRP but not in native PRP. The maximum velocity of healthy subjects and patients on antiplatelet treatment varied significantly as a result of the degree of dilution of the adjusted PRP. Surprisingly, the BCT provided good results when measuring platelet aggregation of native PRP from patients with thrombocytosis, whereas commonly used aggregometers could not analyse platelet aggregation of native PRP in these patients.
Conclusion: The time consuming process of PRP adjustment may not be necessary for platelet aggregation measurements. Moreover, using adjusted PRP for monitoring aspirin or clopidogrel treatment may falsify results. Therefore, it may be better to use native PRP for platelet aggregation measurements, even in patients with thrombocytosis.
Figures

Similar articles
-
Standardization of light transmittance aggregometry for monitoring antiplatelet therapy: an adjustment for platelet count is not necessary.J Thromb Haemost. 2008 Apr;6(4):677-83. doi: 10.1111/j.1538-7836.2008.02891.x. Epub 2008 Jan 8. J Thromb Haemost. 2008. PMID: 18182038
-
To adjust or not to adjust the platelet count in light transmission aggregometry in patients receiving dual aspirin/clopidogrel treatment.Platelets. 2007 Nov;18(7):550-3. doi: 10.1080/09537100701326721. Platelets. 2007. PMID: 17957573 Clinical Trial.
-
Response to aspirin and clopidogrel monitored with different platelet function methods.Platelets. 2006 Aug;17(5):303-10. doi: 10.1080/09537100600746524. Platelets. 2006. PMID: 16928602
-
Aggregometry in the settings of thrombocytopenia, thrombocytosis and antiplatelet therapy.Platelets. 2018 Nov;29(7):644-649. doi: 10.1080/09537104.2018.1445843. Epub 2018 Mar 14. Platelets. 2018. PMID: 29537938 Review.
-
A Systematic Review on the Effect of Common Medications on Platelet Count and Function: Which Medications Should Be Stopped Before Getting a Platelet-Rich Plasma Injection?Orthop J Sports Med. 2022 Apr 12;10(4):23259671221088820. doi: 10.1177/23259671221088820. eCollection 2022 Apr. Orthop J Sports Med. 2022. PMID: 35434168 Free PMC article. Review.
Cited by
-
Intra-articular platelet-rich plasma injections versus intra-articular corticosteroid injections for symptomatic management of knee osteoarthritis: systematic review and meta-analysis.BMC Musculoskelet Disord. 2021 Jun 16;22(1):550. doi: 10.1186/s12891-021-04308-3. BMC Musculoskelet Disord. 2021. PMID: 34134679 Free PMC article.
-
Effects of immunosuppressive agents on the hemostatic system in normal dogs.J Vet Intern Med. 2018 Jul;32(4):1325-1333. doi: 10.1111/jvim.15132. Epub 2018 May 10. J Vet Intern Med. 2018. PMID: 29749651 Free PMC article. Clinical Trial.
-
Effects of pentoxifylline on canine platelet aggregation.Vet Med Sci. 2021 Nov;7(6):2178-2184. doi: 10.1002/vms3.595. Epub 2021 Aug 6. Vet Med Sci. 2021. PMID: 34358418 Free PMC article.
-
Evaluation of participants with suspected heritable platelet function disorders including recommendation and validation of a streamlined agonist panel.Blood. 2012 Dec 13;120(25):5041-9. doi: 10.1182/blood-2012-07-444281. Epub 2012 Sep 21. Blood. 2012. PMID: 23002116 Free PMC article. Clinical Trial.
-
The effects of clopidogrel and omeprazole on platelet function in normal dogs.J Vet Pharmacol Ther. 2017 Apr;40(2):130-139. doi: 10.1111/jvp.12340. Epub 2016 Jul 24. J Vet Pharmacol Ther. 2017. PMID: 27452307 Free PMC article. Clinical Trial.
References
-
- Gachet C. ADP receptors of platelets and their inhibition. Thromb Haemost 2001;86:222–32. - PubMed
-
- Pongracz E. Measurement of platelet aggregation during antiplatelet therapy in ischemic stroke. Clin Hemorheol Microcirc 2004;30:237–42. - PubMed
-
- Moffat KA, Ledford-Kraemer MR, Nichols WL, et al. Variability in clinical laboratory practice in testing for disorders of platelet function. Thromb Haemost 2005;93:549–53. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials