

Axillary apocrine carcinoma with benign apocrine tumours: a case report involving a pathological and immunohistochemical study and review of the literature
- PMID: 15976347
- PMCID: PMC1770727
- DOI: 10.1136/jcp.2004.019794
Axillary apocrine carcinoma with benign apocrine tumours: a case report involving a pathological and immunohistochemical study and review of the literature
Abstract
Background: Apocrine carcinoma is rare and often occurs in the axilla. This is the second apocrine carcinoma arising in bilateral axillae with associated apocrine hyperplasia to be reported.
Aims/methods: Because benign apocrine tumours may be precursors of cancer, this case was investigated immunohistochemically and histologically, and a literature (English and Japanese) review undertaken of cases with coexistent malignant and benign apocrine tumours in the axilla to elucidate the relation between apocrine carcinoma and benign apocrine tumours.
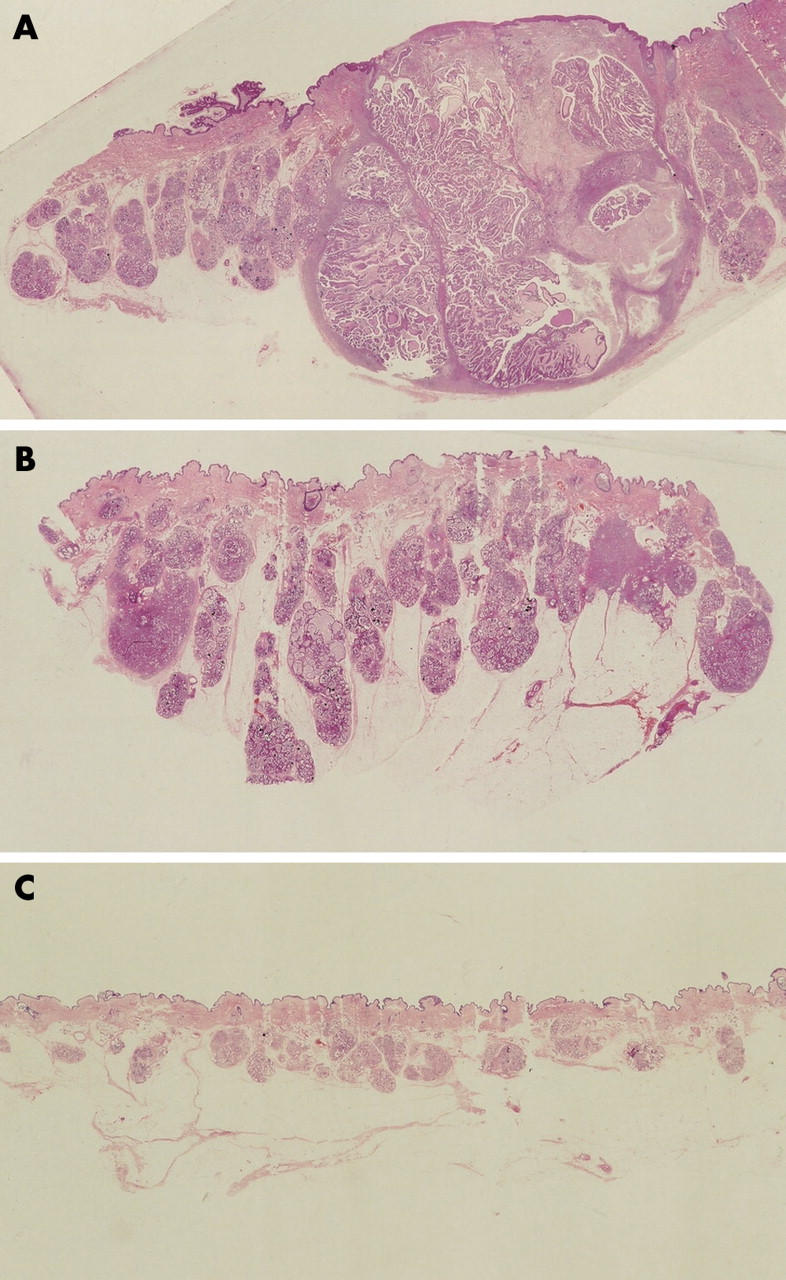
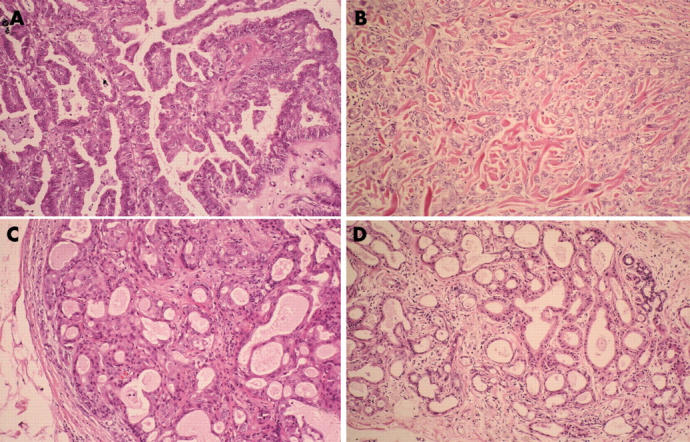
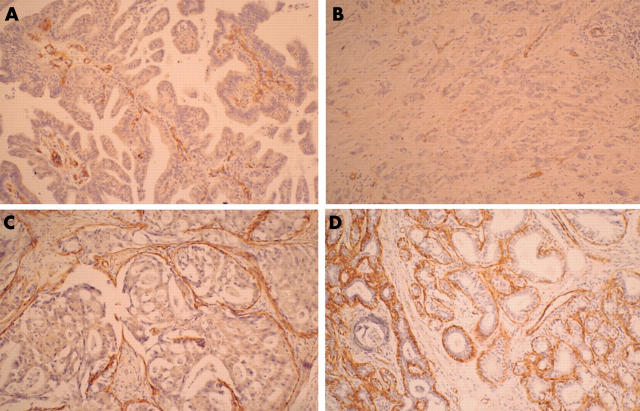
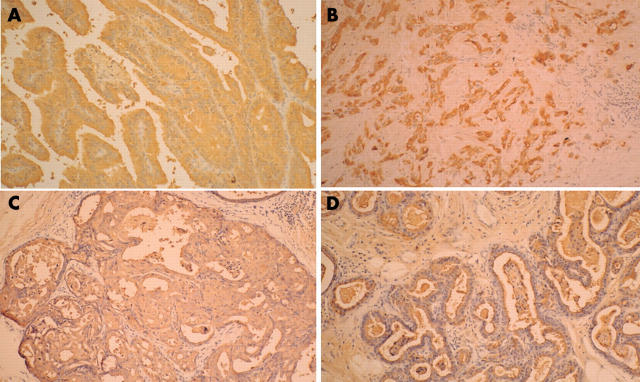
Results: Only four cases of axillary apocrine carcinoma with benign apocrine tumours were identified in the literature. In each case, benign apocrine hyperplasia was situated within and surrounding the adenocarcinomatous nests. Staining for epithelial membrane antigen revealed three patterns: (1) poorly differentiated tumour cells showing strong cytoplasmic staining; (2) combined luminal surface and cytoplasmic staining of glandular cells; and (3) a strongly positive lineal staining pattern at the luminal membrane surface, comprising one or two apocrine hyperplastic secretory cells. The basal lesions of apocrine hyperplasia were strongly positive for alpha smooth muscle actin, whereas the periphery of adenomatous lesions showed weaker positive staining, even though the periphery of adenocarcinomatous lesions was negative.
Conclusions: All five apocrine carcinomas with benign apocrine tumours occurred in elderly Japanese men who had bilateral benign apocrine tumours even if affected by unilateral axillary apocrine carcinoma. The immunohistochemical results support the notion that apocrine hyperplasia is a precursor of cancer and that apocrine carcinoma, adenoma, and hyperplasia may be successive steps in the linear progression to carcinoma.
Figures
References
-
- Murphy GF, Elder DE. Apocrine adenocarcinoma. In: Rosai J, Sobin LH, eds. Atlas of tumor pathology. Non-melanocytic tumors of the skin. Washington, DC: Armed Forces Institute of Pathology, 1990:119–20.
-
- Chamberlain RS, Huber K, White JC, et al. Apocrine gland carcinoma of the axilla. Review of the literature and recommendations for treatment. Am J Clin Oncol 1999;22:131–5. - PubMed
-
- Kage M, Nakamura Y, Ozumi K. A case report of equivocal neoplasm originating from an apocrine gland on the eyelid. Acta Pathol Jpn 1990;40:431–4. - PubMed
-
- Shintaku M, Tsuta K, Yoshida H, et al. Apocrine adenocarcinoma of the eyelid with aggressive biological behavior: report of a case. Pathol Int 2002;52:169–73. - PubMed
-
- Yoshida A, Kodama Y, Hatanaka S, et al. Apocrine adenocarcinoma of the bilateral axillae. Acta Pathol Jpn 1991;41:927–32. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources