

Methods of hysterectomy: systematic review and meta-analysis of randomised controlled trials
- PMID: 15976422
- PMCID: PMC558455
- DOI: 10.1136/bmj.330.7506.1478
Methods of hysterectomy: systematic review and meta-analysis of randomised controlled trials
Abstract
Objective: To evaluate the most appropriate surgical method of hysterectomy (abdominal, vaginal, or laparoscopic) for women with benign disease.
Design: Systematic review and meta-analysis.
Data sources: Cochrane Menstrual Disorders and Subfertility Group Trials Register, Cochrane Central Register of Controlled Trials, Medline, Embase, and Biological Abstracts.
Selection of studies: Only randomised controlled trials were selected; participants had to have benign gynaecological disease; interventions had to comprise at least one hysterectomy method compared with another; and trials had to report primary outcomes (time taken to return to normal activities, intraoperative visceral injury, and major long term complications) or secondary outcomes (operating time, other immediate complications of surgery, short term complications, and duration of hospital stay).
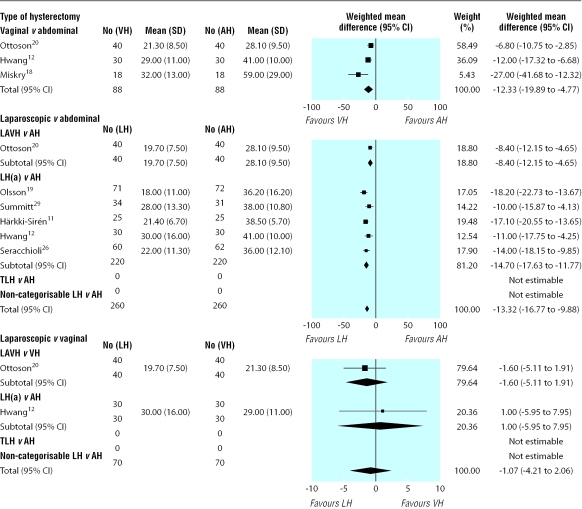
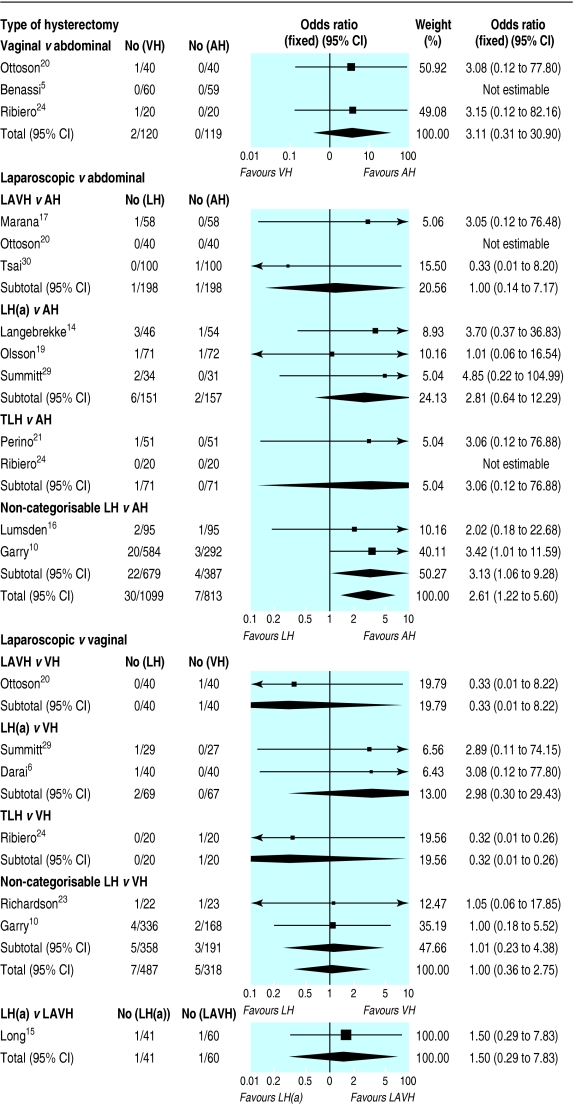
Results: 27 trials (total of 3643 participants) were included. Return to normal activities was quicker after vaginal than after abdominal hysterectomy (weighted mean difference 9.5 (95% confidence interval 6.4 to 12.6) days) and after laparoscopic than after abdominal hysterectomy (difference 13.6 (11.8 to 15.4) days), but was not significantly different for laparoscopic versus vaginal hysterectomy (difference -1.1 (-4.2 to 2.1) days). There were more urinary tract injuries with laparoscopic than with abdominal hysterectomy (odds ratio 2.61 (95% confidence interval 1.22 to 5.60)), but no other intraoperative visceral injuries showed a significant difference between surgical approaches. Data were notably absent for many important long term patient outcome measures, where the analyses were underpowered to detect important differences, or they were simply not reported in trials.
Conclusions: Significantly speedier return to normal activities and other improved secondary outcomes (shorter duration of hospital stay and fewer unspecified infections or febrile episodes) suggest that vaginal hysterectomy is preferable to abdominal hysterectomy where possible. Where vaginal hysterectomy is not possible, laparoscopic hysterectomy is preferable to abdominal hysterectomy, although it brings a higher chance of bladder or ureter injury.
Figures
Comment in
-
Hysterectomy for benign conditions.BMJ. 2005 Jun 25;330(7506):1457-8. doi: 10.1136/bmj.330.7506.1457. BMJ. 2005. PMID: 15976393 Free PMC article. No abstract available.
-
Methods of hysterectomy: should women have a say?BMJ. 2005 Aug 6;331(7512):351-2. doi: 10.1136/bmj.331.7512.351-b. BMJ. 2005. PMID: 16081455 Free PMC article. No abstract available.
Similar articles
-
Surgical approach to hysterectomy for benign gynaecological disease.Cochrane Database Syst Rev. 2006 Apr 19;(2):CD003677. doi: 10.1002/14651858.CD003677.pub3. Cochrane Database Syst Rev. 2006. Update in: Cochrane Database Syst Rev. 2009 Jul 08;(3):CD003677. doi: 10.1002/14651858.CD003677.pub4. PMID: 16625589 Updated.
-
Surgical approach to hysterectomy for benign gynaecological disease.Cochrane Database Syst Rev. 2005 Jan 25;(1):CD003677. doi: 10.1002/14651858.CD003677.pub2. Cochrane Database Syst Rev. 2005. Update in: Cochrane Database Syst Rev. 2006 Apr 19;(2):CD003677. doi: 10.1002/14651858.CD003677.pub3. PMID: 15674911 Updated.
-
Surgical approach to hysterectomy for benign gynaecological disease.Cochrane Database Syst Rev. 2009 Jul 8;(3):CD003677. doi: 10.1002/14651858.CD003677.pub4. Cochrane Database Syst Rev. 2009. Update in: Cochrane Database Syst Rev. 2015 Aug 12;(8):CD003677. doi: 10.1002/14651858.CD003677.pub5. PMID: 19588344 Updated.
-
Laparoscopic colposuspension for urinary incontinence in women.Cochrane Database Syst Rev. 2006 Jul 19;(3):CD002239. doi: 10.1002/14651858.CD002239.pub2. Cochrane Database Syst Rev. 2006. PMID: 16855989
-
Sertindole for schizophrenia.Cochrane Database Syst Rev. 2005 Jul 20;2005(3):CD001715. doi: 10.1002/14651858.CD001715.pub2. Cochrane Database Syst Rev. 2005. PMID: 16034864 Free PMC article.
Cited by
-
Transvaginal specimen removal after laparoscopic distal pancreatic resection.Langenbecks Arch Surg. 2013 Oct;398(7):1001-5. doi: 10.1007/s00423-013-1092-3. Epub 2013 Jun 13. Langenbecks Arch Surg. 2013. PMID: 23760755
-
Preemptive pregabalin for postoperative analgesia during minimally invasive hysterectomy: a systematic review and meta-analysis of randomized controlled trials.Obstet Gynecol Sci. 2022 Mar;65(2):133-144. doi: 10.5468/ogs.21345. Epub 2022 Feb 23. Obstet Gynecol Sci. 2022. PMID: 35193327 Free PMC article.
-
Laparoendoscopic single-site versus conventional laparoscopic-assisted vaginal hysterectomy for benign or pre-invasive uterine disease.Surg Endosc. 2015 Apr;29(4):890-7. doi: 10.1007/s00464-014-3747-8. Epub 2014 Aug 9. Surg Endosc. 2015. PMID: 25106721
-
Pedagogic Approach in the Surgical Learning: The First Period of "Assistant Surgeon" May Improve the Learning Curve for Laparoscopic Robotic-Assisted Hysterectomy.Front Surg. 2016 Nov 2;3:58. doi: 10.3389/fsurg.2016.00058. eCollection 2016. Front Surg. 2016. PMID: 27853733 Free PMC article.
-
A new approach to simplify surgical colpotomy in laparoscopic hysterectomy.Gynecol Surg. 2016;13:63-69. doi: 10.1007/s10397-015-0929-x. Epub 2016 Jan 12. Gynecol Surg. 2016. PMID: 26918004 Free PMC article.
References
-
- Garry R, Reich H, Liu CY. Laparoscopic hysterectomy—definitions and indications. Gynaecol Endosc 1994;3: 1-3.
-
- Garry R. Towards evidence-based hysterectomy. Gynaecol Endosc 1998;7: 225-33.
-
- Reich H, Roberts L. Laparoscopic hysterectomy in current gynaecological practice. Rev Gynaecol Pract 2003;3: 32-40.
-
- Johnson N, Barlow D, Lethaby A, Tavender E, Curr E, Garry R. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev 2005;(2): CD003677. - PubMed
-
- Benassi L, Rossi T, Kaihura CT, Ricci L, Bedocchi L, Galanti B. Abdominal or vaginal hysterectomy for enlarged uteri: a randomized clinical trial. Am J Obstet Gynecol 2002;187: 1561-5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials