

Review
doi: 10.1136/bmj.330.7506.1493.
Radiological review of pneumothorax
Affiliations
- PMID: 15976424
- PMCID: PMC558461
- DOI: 10.1136/bmj.330.7506.1493
Item in Clipboard
Review
Radiological review of pneumothorax
BMJ.
.
No abstract available
Figures
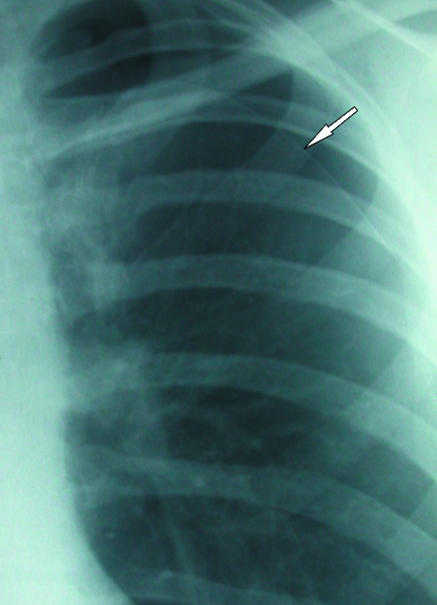
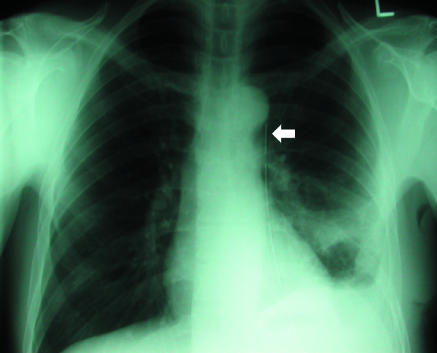
(left) Classic appearances of left sided pneumothorax with readily apparent visceral pleural line (arrow)
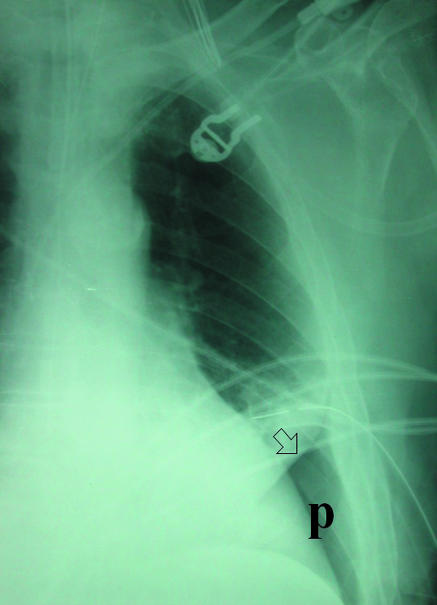
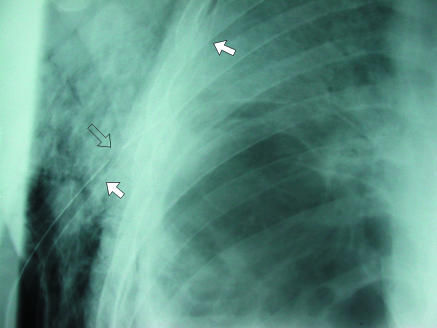
(right) Supine projection showing air collected at lung base. Absent lung markings and a visceral pleural line (arrow) are still visible (P=pneumothorax). Left basal chest drain is noted
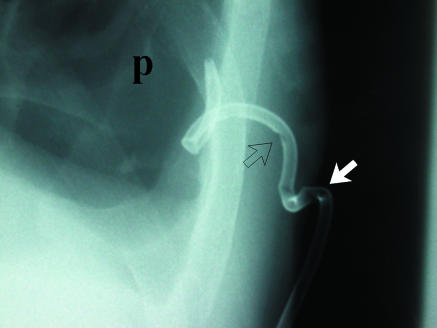
(left) Loculated left sided pneumothorax in a patient with severe chronic obstructive airways disease. Placement of chest drain into fifth intercostal space (arrow) might have entered lung parenchyma and would most likely not have achieved complete drainage of this loculated collection. (right) Percutaneous pigtail catheters (arrows) placed in apical and basal components of pneumothorax under fluoroscopic guidance. After several days of drainage the lung re-expanded completely

(left) Loculated left sided pneumothorax in a patient with severe chronic obstructive airways disease. Placement of chest drain into fifth intercostal space (arrow) might have entered lung parenchyma and would most likely not have achieved complete drainage of this loculated collection. (right) Percutaneous pigtail catheters (arrows) placed in apical and basal components of pneumothorax under fluoroscopic guidance. After several days of drainage the lung re-expanded completely
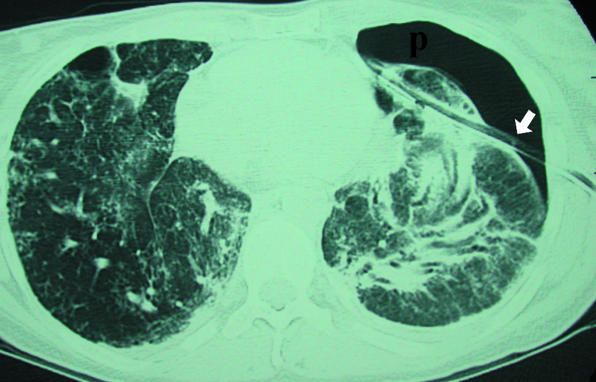
Extensive pulmonary fibrosis and left pneumothorax (p) treated by blind chest drain placement. Axial computed tomograpy shows that drain (arrow) has traversed lung parenchyma. This led to a deterioration in patient's clinical condition
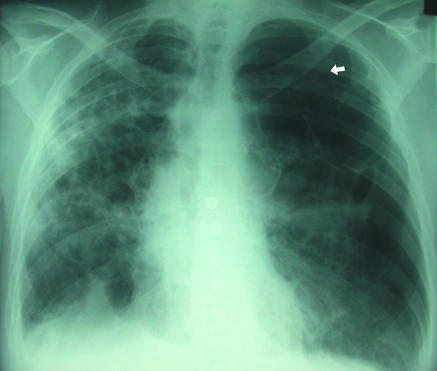
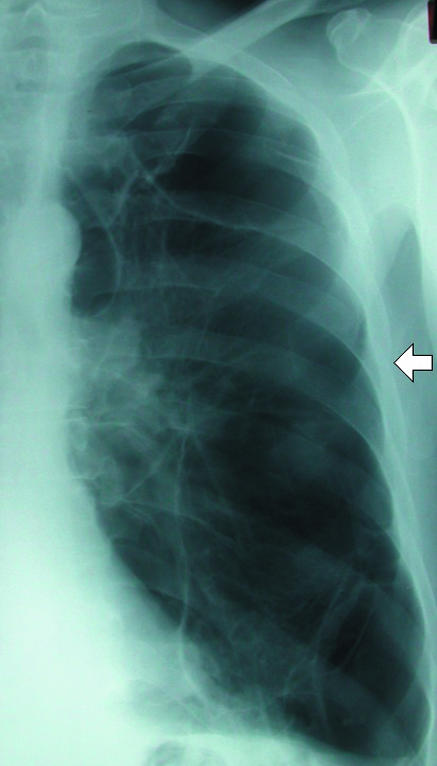
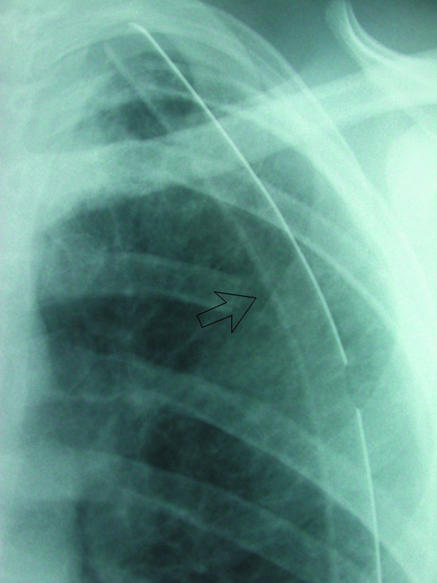
Background fibrotic lung disease (underlying ulcerative colitis), which places patient at risk of secondary pneumothorax. Although medial border of scapula (arrow) is easily recognisable as such on this radiograph it can sometimes be misinterpreted as a visceral pleural line
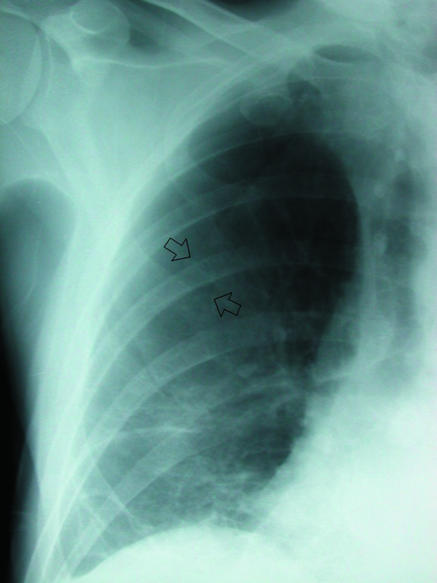
(left) Skin folds (arrows) overlying right hemithorax. Distal lung markings are readily apparent. Note folds are relatively straight unlike curved visceral pleural line of pneumothorax
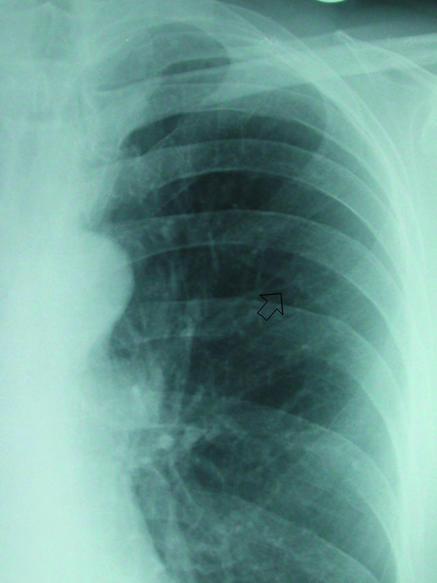
(right) Prominent companion or accompanying shadow below left sixth rib (arrow). Line is relatively parallel to accompanying rib, and distal lung markings are evident
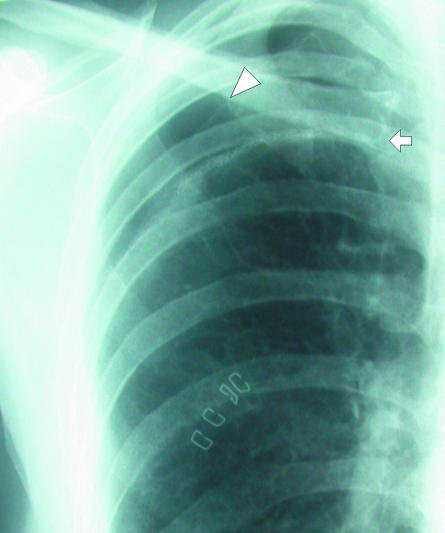
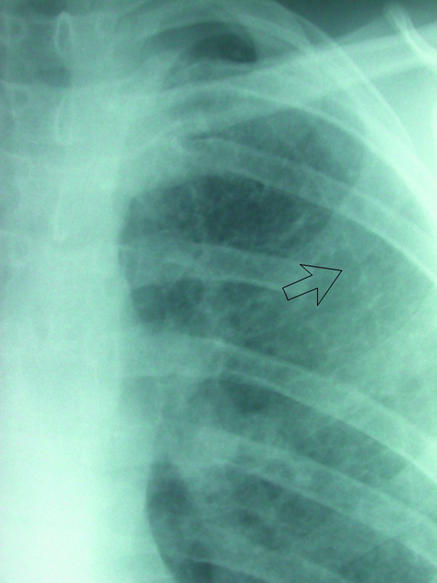
This patient underwent pleurectomy for recurrent pneumothorax. Suture material at right apex (arrow) is thicker than visceral pleural line and should not be confused with recurrent air leak. Compare with adjacent apical pneumothorax (arrowhead)
(top) Chest radiography shows unremarkable appearance of intercostal drain (arrow), apart from its medial location. (bottom) Axial computed tomography shows drain (arrow) is located in subcutaneous tissues. More superior images showed that the drain terminated in this superficial position

(top) Chest radiography shows unremarkable appearance of intercostal drain (arrow), apart from its medial location. (bottom) Axial computed tomography shows drain (arrow) is located in subcutaneous tissues. More superior images showed that the drain terminated in this superficial position
(top) Two large bore chest drains in a patient who developed a pneumothorax secondary to cavitating pneumonia. Lower drain (white arrows) is satisfactorily sited, but upper drain (open arrow) has side holes protruding into subcutaneous tissues, leading to extensive air leak. (bottom) Small pigtail catheter inserted into basal pneumothorax (p). Progressive traction on drain has led to extrusion of side holes into subcutaneous tissues (open arrow) and through skin surface (white arrow)
(top) Two large bore chest drains in a patient who developed a pneumothorax secondary to cavitating pneumonia. Lower drain (white arrows) is satisfactorily sited, but upper drain (open arrow) has side holes protruding into subcutaneous tissues, leading to extensive air leak. (bottom) Small pigtail catheter inserted into basal pneumothorax (p). Progressive traction on drain has led to extrusion of side holes into subcutaneous tissues (open arrow) and through skin surface (white arrow)
(left) Left apical chest drain (open arrow) in satisfactory position after lobectomy. (right) Chest radiograph after removal of drain next day shows faint radio-opaque line (arrow), known as a “drain track.” This was seen to resolve on subsequent radiographs
(left) Left apical chest drain (open arrow) in satisfactory position after lobectomy. (right) Chest radiograph after removal of drain next day shows faint radio-opaque line (arrow), known as a “drain track.” This was seen to resolve on subsequent radiographs
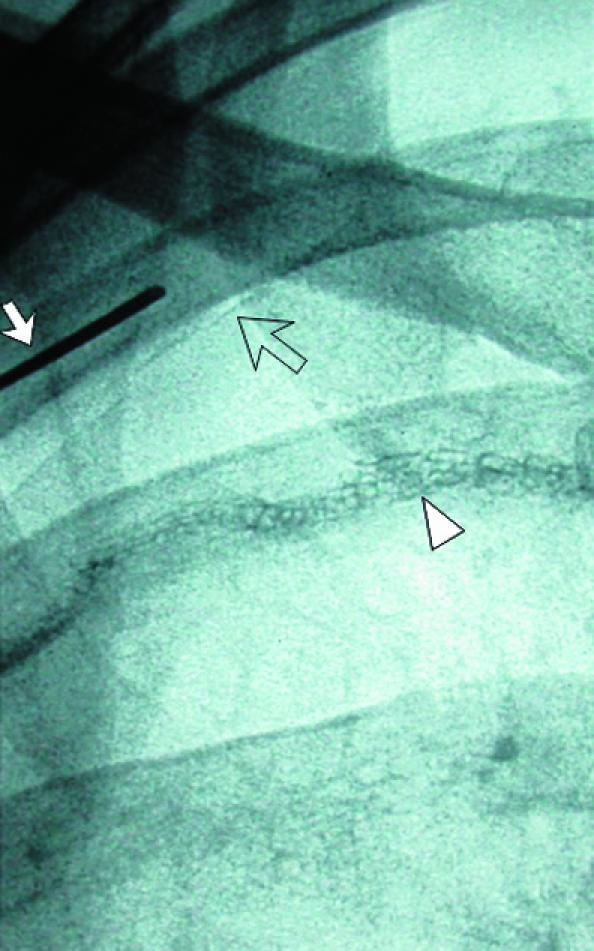
(left) Small pneumothorax post-pleurectomy at right apex (open arrow). Fluoroscopic guided needle puncture (white arrow) is being carried out. This unusual approach through the first intercostal space could damage subclavian vessels, which can be avoided by preliminary ultrasound examination of the needle path (arrowhead=suture material). (centre) Wire (arrow) is placed through the needle after aspiration of air. (right) Pigtail catheter coiled in pneumothorax and connected to underwater seal
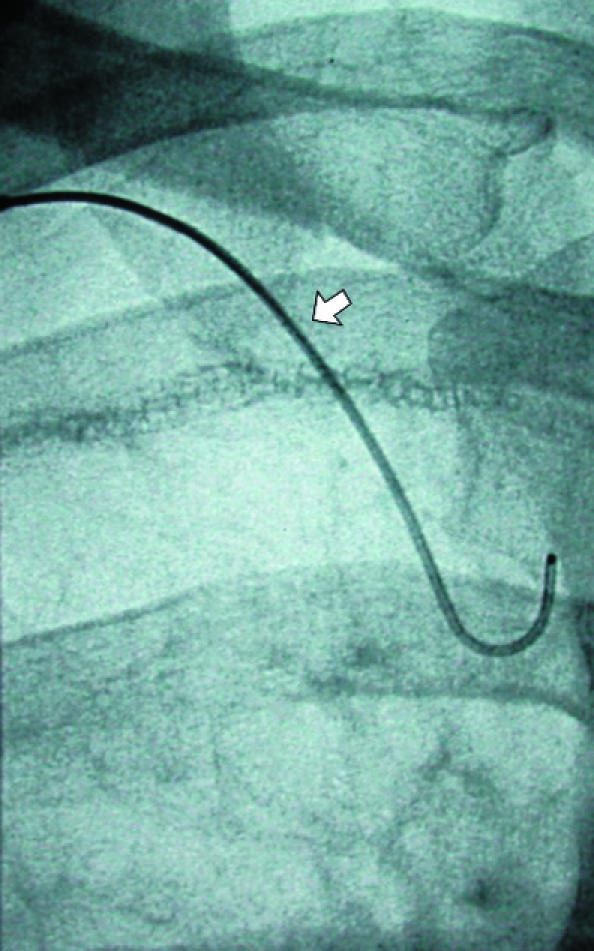
(left) Small pneumothorax post-pleurectomy at right apex (open arrow). Fluoroscopic guided needle puncture (white arrow) is being carried out. This unusual approach through the first intercostal space could damage subclavian vessels, which can be avoided by preliminary ultrasound examination of the needle path (arrowhead=suture material). (centre) Wire (arrow) is placed through the needle after aspiration of air. (right) Pigtail catheter coiled in pneumothorax and connected to underwater seal
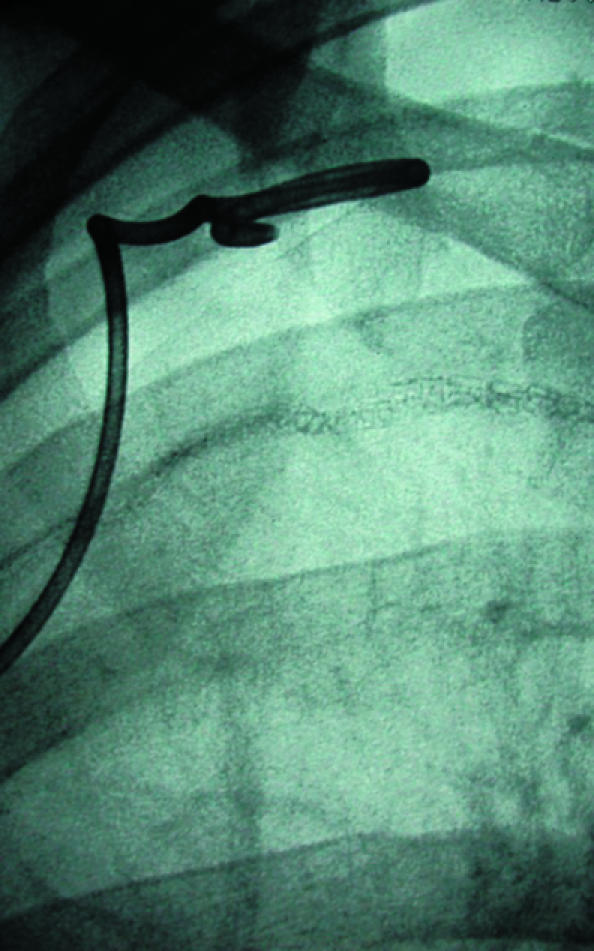
(left) Small pneumothorax post-pleurectomy at right apex (open arrow). Fluoroscopic guided needle puncture (white arrow) is being carried out. This unusual approach through the first intercostal space could damage subclavian vessels, which can be avoided by preliminary ultrasound examination of the needle path (arrowhead=suture material). (centre) Wire (arrow) is placed through the needle after aspiration of air. (right) Pigtail catheter coiled in pneumothorax and connected to underwater seal
References
-
- Melton LJ, Hepper NG, Offord KP. Incidence of spontaneous pneumothorax in Olmsted County, Minnesota: 1950 to 1974. Am Rev Respir Dis 1979;120: 1379-82. - PubMed
-
- Glazer H, Anderson DJ, Wilson BS, Molin PL, Sagel SS. Pneumothorax: appearances on lateral chest radiographs. Radiology 1989;173: 707-11. - PubMed
-
- Seow A, Kazerooni EA, Pernicano PG, Neary M. Comparison of upright inspiratory and expiratory chest radiographs for detecting pneumothoraces. Am J Roentgenol 1996;166: 313-6. - PubMed
-
- Kurihara Y, Yakushiji YK, Matsumoto J, Ishikawa T, Hirata K. The ribs: anatomic and radiologic considerations. Radiographics 1999;19: 105-19;151-2. [Quiz.] - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical