

Mediastinoscopy in the treatment of mediastinal cysts
- PMID: 15984700
- PMCID: PMC3015566
Mediastinoscopy in the treatment of mediastinal cysts
Abstract
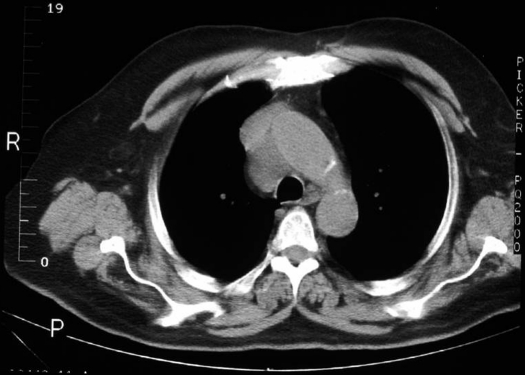
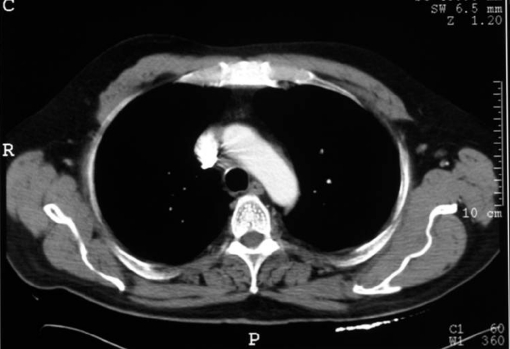
Objective: Primary cysts constitute 25% of all masses in the mediastinum. Because radiological investigations are often inconclusive, many adults require mediastinoscopy, thoracotomy, video-assisted thoracic surgery, or computed tomography-guided transbronchial, transesophageal, or transcutaneous aspiration to confirm the cystic nature of these lesions. Minimally invasive procedures fail when the cyst contents are gelatinous and mucoid (failure to aspirate) or when the cyst wall continues to secrete fluid. Though Pursel reported mediastinoscopic extirpation of benign cysts 35 years ago, it remains a "therapeutic curiosity" with sporadic reports of its usage. We report 2 successful mediastinal cyst extirpations performed as outpatient procedures and review the literature with regards to its management.
Methods: A rigid, 8-mm mediastinoscope was inserted into the anterior mediastinum following the creation of a 2-cm suprasternal incision and dissection along the anterior surface of the trachea. After aspiration, cytology of the contents revealed their benign nature. Right paratracheal cysts in 2 adult males were successfully removed mediastinoscopically by blunt and sharp dissection.
Results: Histopathology revealed benign mesothelial cysts in both instances. Both patients had an uncomplicated procedure and were discharged within 23 hours. No other pathology was detected on mediastinoscopy, and follow-up at 3 months and 6 months has revealed no recurrence.
Conclusion: Mediastinoscopic cyst removal is a minimally invasive procedure with a very low morbidity and mortality rate. Morbidity, recovery, and discharge times are much less than those of more invasive procedures (video-assisted thoracic surgery / thoracotomy). We suggest that it should be the first-choice procedure for the excision of appropriately located benign mediastinal cysts.
Figures


References
-
- Burkell CC, Cross JM, Kent HP, Nanson EM. Mass lesions of mediastinum. Curr Probl Surg. June 1969;2–57 - PubMed
-
- Davis RD, Oldham HN, Sabiston DC. Primary cysts and neoplasms of the mediastinum: Recent changes in clinical presentation, methods of diagnosis, management, and results. Ann Thorac Surg. 1987;44:229–237 - PubMed
-
- Petkar M, Vaideeswar P, Deshpande JR, et al. Surgical pathology of cystic lesions of the mediastinum. J Postgrad Med. 2001;47(4):235–239 - PubMed
-
- Salyer DC, Salyer WR, Eggleston JC. Benign developmental cysts of the mediastinum. Arch Pathol Lab Med. 1977;101:136–139 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources