

The central role of vascular extracellular matrix and basement membrane remodeling in metabolic syndrome and type 2 diabetes: the matrix preloaded
- PMID: 15985157
- PMCID: PMC1175853
- DOI: 10.1186/1475-2840-4-9
The central role of vascular extracellular matrix and basement membrane remodeling in metabolic syndrome and type 2 diabetes: the matrix preloaded
Abstract
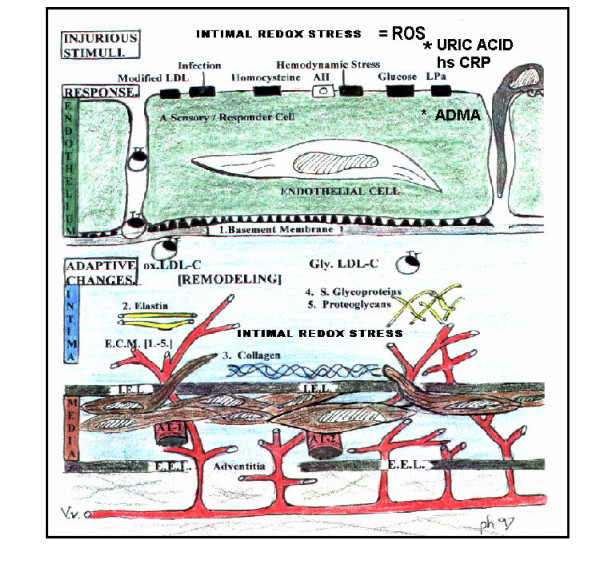
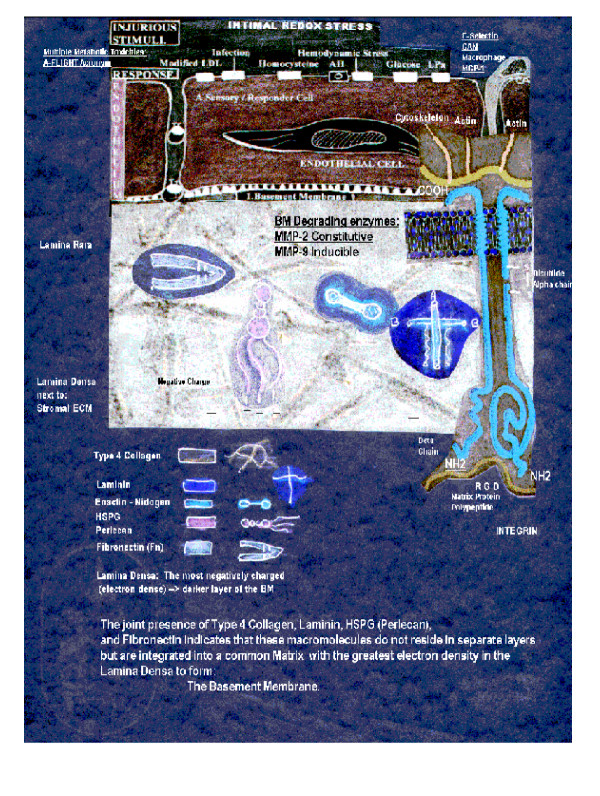
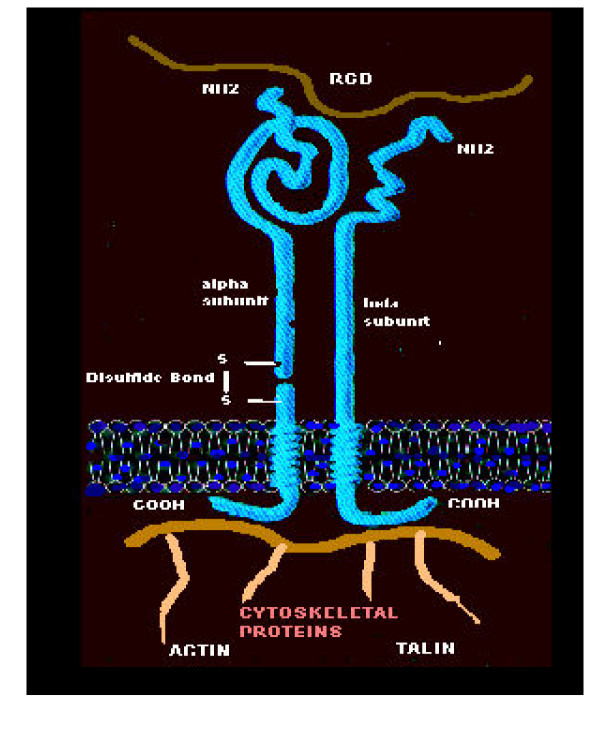
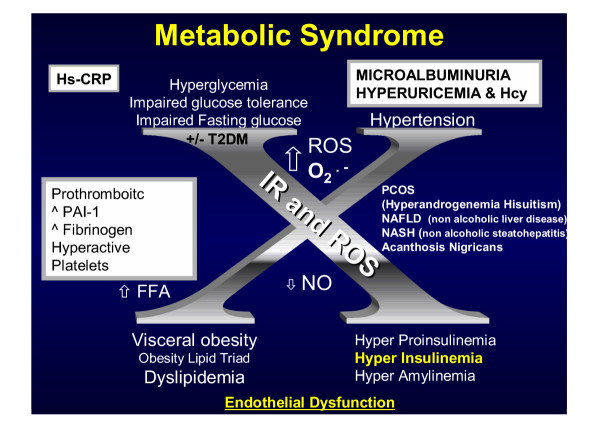
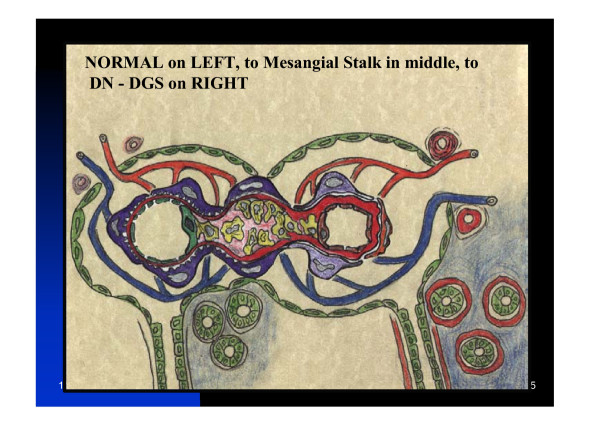
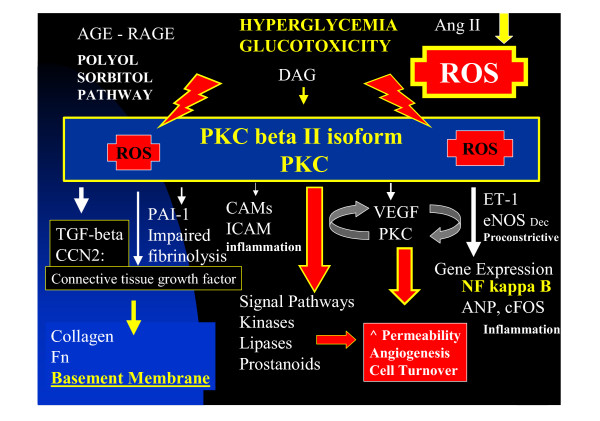
The vascular endothelial basement membrane and extra cellular matrix is a compilation of different macromolecules organized by physical entanglements, opposing ionic charges, chemical covalent bonding, and cross-linking into a biomechanically active polymer. These matrices provide a gel-like form and scaffolding structure with regional tensile strength provided by collagens, elasticity by elastins, adhesiveness by structural glycoproteins, compressibility by proteoglycans--hyaluronans, and communicability by a family of integrins, which exchanges information between cells and between cells and the extracellular matrix of vascular tissues. Each component of the extracellular matrix and specifically the capillary basement membrane possesses unique structural properties and interactions with one another, which determine the separate and combined roles in the multiple diabetic complications or diabetic opathies. Metabolic syndrome, prediabetes, type 2 diabetes mellitus, and their parallel companion (atheroscleropathy) are associated with multiple metabolic toxicities and chronic injurious stimuli. The adaptable quality of a matrix or form genetically preloaded with the necessary information to communicate and respond to an ever-changing environment, which supports the interstitium, capillary and arterial vessel wall is individually examined.
Figures
Similar articles
-
Basic components of connective tissues and extracellular matrix: elastin, fibrillin, fibulins, fibrinogen, fibronectin, laminin, tenascins and thrombospondins.Adv Exp Med Biol. 2014;802:31-47. doi: 10.1007/978-94-007-7893-1_3. Adv Exp Med Biol. 2014. PMID: 24443019 Review.
-
Fibrillar, fibril-associated and basement membrane collagens of the arterial wall: architecture, elasticity and remodeling under stress.Curr Pharm Des. 2015;21(9):1124-33. doi: 10.2174/1381612820666141013122906. Curr Pharm Des. 2015. PMID: 25312736 Review.
-
Microvascular basement membranes in diabetes mellitus.J Pathol. 2003 Jul;200(4):537-46. doi: 10.1002/path.1439. J Pathol. 2003. PMID: 12845621 Review.
-
Vascular ossification-calcification in metabolic syndrome, type 2 diabetes mellitus, chronic kidney disease, and calciphylaxis-calcific uremic arteriolopathy: the emerging role of sodium thiosulfate.Cardiovasc Diabetol. 2005 Mar 18;4:4. doi: 10.1186/1475-2840-4-4. Cardiovasc Diabetol. 2005. PMID: 15777477 Free PMC article. Review.
-
Reorganization of basement membrane matrices by cellular traction promotes the formation of cellular networks in vitro.Lab Invest. 1992 May;66(5):536-47. Lab Invest. 1992. PMID: 1374138
Cited by
-
Deficient Leptin Cellular Signaling Plays a Key Role in Brain Ultrastructural Remodeling in Obesity and Type 2 Diabetes Mellitus.Int J Mol Sci. 2021 May 21;22(11):5427. doi: 10.3390/ijms22115427. Int J Mol Sci. 2021. PMID: 34063911 Free PMC article. Review.
-
Training differentially regulates elastin level and proteolysis in skeletal and heart muscles and aorta in healthy rats.Biol Open. 2016 May 15;5(5):556-62. doi: 10.1242/bio.017459. Biol Open. 2016. PMID: 27069251 Free PMC article.
-
Type 2 Diabetes Mellitus Increases The Risk of Late-Onset Alzheimer's Disease: Ultrastructural Remodeling of the Neurovascular Unit and Diabetic Gliopathy.Brain Sci. 2019 Sep 29;9(10):262. doi: 10.3390/brainsci9100262. Brain Sci. 2019. PMID: 31569571 Free PMC article. Review.
-
Senescent endothelial cells: a potential target for diabetic retinopathy.Angiogenesis. 2024 Nov;27(4):663-679. doi: 10.1007/s10456-024-09943-7. Epub 2024 Aug 31. Angiogenesis. 2024. PMID: 39215875 Free PMC article. Review.
-
Long-term phosphodiesterase 5 inhibitor administration reduces inflammatory markers and heat-shock proteins in cavernous tissue of Zucker diabetic fatty rat (ZDF/fa/fa).Int J Impot Res. 2015 Sep-Oct;27(5):182-90. doi: 10.1038/ijir.2015.13. Epub 2015 Jul 23. Int J Impot Res. 2015. PMID: 26202338
References
-
- Siperstein MD, Unger RH, Madison LL. Further electron microscopic studies of diabetic microangiopathy. Adv Metab Disord. 1970;1:261. - PubMed
-
- Merimee TJ, Siperstein MD, Fineberg SE, McKusick VA. The microangiopathic lesions of diabetes mellitus: an evaluation of possible causative factors. Trans Assoc Am Physicians. 1970;83:102–112. - PubMed
-
- Siperstein MD. Capillary basement membranes and diabetic microangiopathy. Adv Intern Med. 1972;18:325–344. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
