

A dynamic neuro-fuzzy model providing bio-state estimation and prognosis prediction for wearable intelligent assistants
- PMID: 15985181
- PMCID: PMC1182386
- DOI: 10.1186/1743-0003-2-15
A dynamic neuro-fuzzy model providing bio-state estimation and prognosis prediction for wearable intelligent assistants
Abstract
Background: Intelligent management of wearable applications in rehabilitation requires an understanding of the current context, which is constantly changing over the rehabilitation process because of changes in the person's status and environment. This paper presents a dynamic recurrent neuro-fuzzy system that implements expert-and evidence-based reasoning. It is intended to provide context-awareness for wearable intelligent agents/assistants (WIAs).
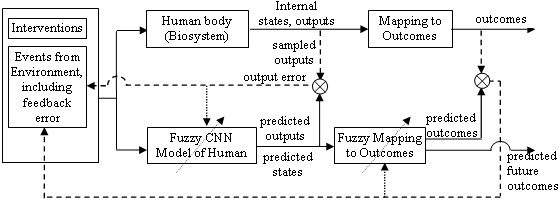
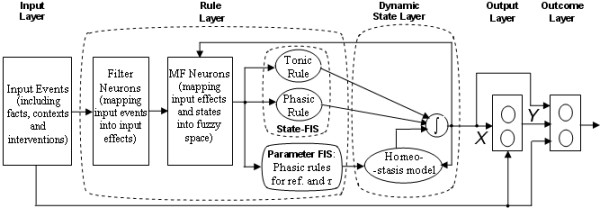
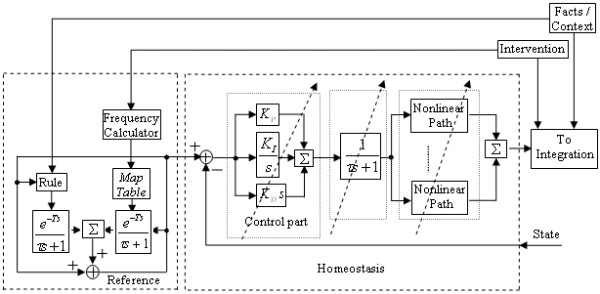
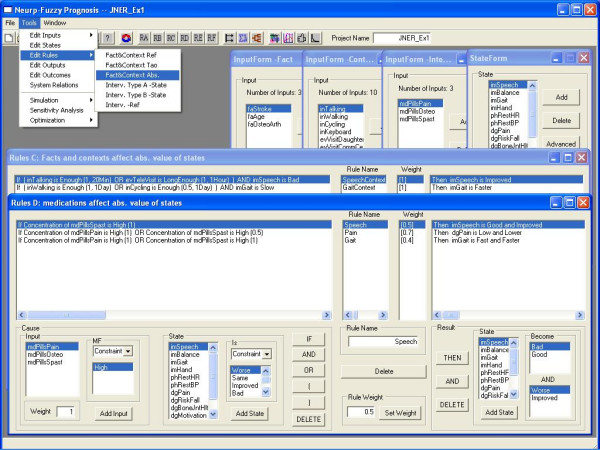
Methods: The model structure includes the following types of signals: inputs, states, outputs and outcomes. Inputs are facts or events which have effects on patients' physiological and rehabilitative states; different classes of inputs (e.g., facts, context, medication, therapy) have different nonlinear mappings to a fuzzy "effect." States are dimensionless linguistic fuzzy variables that change based on causal rules, as implemented by a fuzzy inference system (FIS). The FIS, with rules based on expertise and evidence, essentially defines the nonlinear state equations that are implemented by nuclei of dynamic neurons. Outputs, a function of weighing of states and effective inputs using conventional or fuzzy mapping, can perform actions, predict performance, or assist with decision-making. Outcomes are scalars to be extremized that are a function of outputs and states.
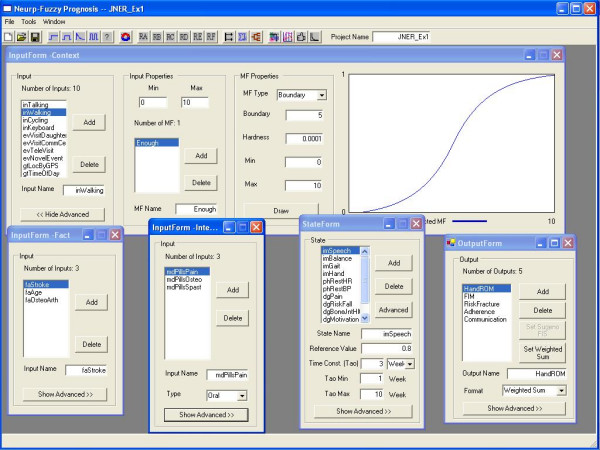
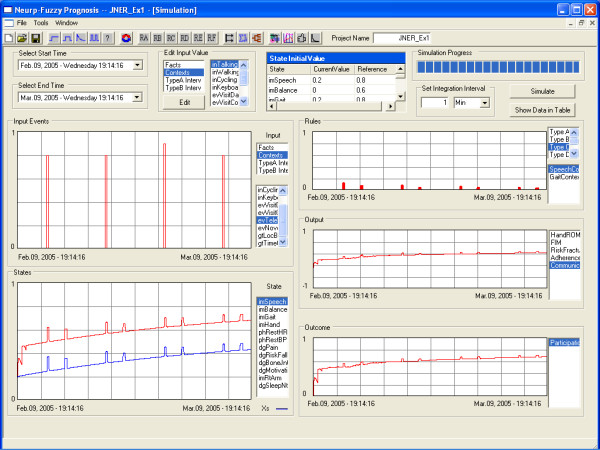
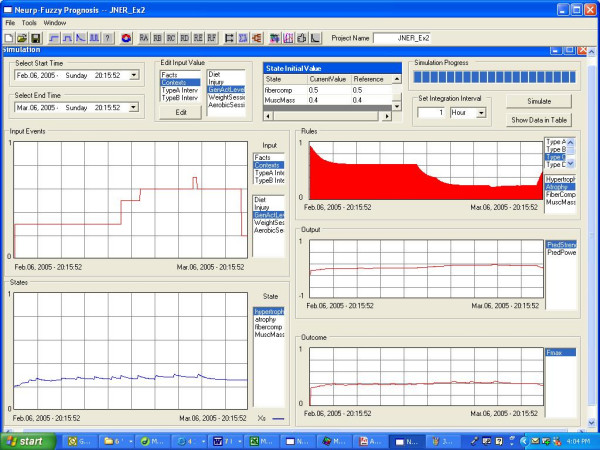
Results: The first example demonstrates setup and use for a large-scale stroke neurorehabilitation application (with 16 inputs, 12 states, 5 outputs and 3 outcomes), showing how this modelling tool can successfully capture causal dynamic change in context-relevant states (e.g., impairments, pain) as a function of input event patterns (e.g., medications). The second example demonstrates use of scientific evidence to develop rule-based dynamic models, here for predicting changes in muscle strength with short-term fatigue and long-term strength-training.
Conclusion: A neuro-fuzzy modelling framework is developed for estimating rehabilitative change that can be applied in any field of rehabilitation if sufficient evidence and/or expert knowledge are available. It is intended to provide context-awareness of changing status through state estimation, which is critical information for WIA's to be effective.
Figures
Similar articles
-
Development of river ecosystem models for Flemish watercourses: case studies in the Zwalm river basin.Meded Rijksuniv Gent Fak Landbouwkd Toegep Biol Wet. 2001;66(1):71-86. Meded Rijksuniv Gent Fak Landbouwkd Toegep Biol Wet. 2001. PMID: 15952431
-
Fuzzy jump wavelet neural network based on rule induction for dynamic nonlinear system identification with real data applications.PLoS One. 2019 Dec 9;14(12):e0224075. doi: 10.1371/journal.pone.0224075. eCollection 2019. PLoS One. 2019. PMID: 31816627 Free PMC article.
-
eFSM--a novel online neural-fuzzy semantic memory model.IEEE Trans Neural Netw. 2010 Jan;21(1):136-57. doi: 10.1109/TNN.2009.2035116. Epub 2009 Dec 11. IEEE Trans Neural Netw. 2010. PMID: 20007031
-
Industrial application of fuzzy control in bioprocesses.Adv Biochem Eng Biotechnol. 2004;87:151-71. doi: 10.1007/b13535. Adv Biochem Eng Biotechnol. 2004. PMID: 15217106 Review.
-
Trainable fusion rules. I. Large sample size case.Neural Netw. 2006 Dec;19(10):1506-16. doi: 10.1016/j.neunet.2006.01.018. Epub 2006 Apr 3. Neural Netw. 2006. PMID: 16580815 Review.
References
-
- Winters JM. Emerging rehabilitative telehealthcare anywhere. Was the Homecare Technologies Workshop visionary? In: Winters JM, Robinson C, Simpson R, Vanderheiden G, editor. Emerging and Accessible Telecommunications, Information and Healthcare Technologies. Arlington: RESNA Press; 2002. pp. 95–111.
-
- Winters JM, Herman W. Report of the Workshop on Home Care Technologies for the 21st Century. Catholic University of America, Washington DC Tech Rep HCTR-10-v10. 2000. p. 96.http://www.eng.mu.edu/wintersj/HCTWorkshop
-
- Winters JM. Mobile telerehabilitative healthcare technologies. In: Rosen MJ, Lauderdale D, editor. Proceedings of the state of the science conference on telerehabiliation and application of virtual reality. Washington DC: NRH Press; 2001. pp. 102–108.
-
- American Physical Therapy Association Guide to Physical Therapist Practice. 1997. ch1.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
