

Toward optimal screening strategies for older women. Costs, benefits, and harms of breast cancer screening by age, biology, and health status
- PMID: 15987322
- PMCID: PMC1490138
- DOI: 10.1111/j.1525-1497.2005.0116.x
Toward optimal screening strategies for older women. Costs, benefits, and harms of breast cancer screening by age, biology, and health status
Abstract
Context: Optimal ages of breast cancer screening cessation remain uncertain.
Objective: To evaluate screening policies based on age and quartiles of life expectancy (LE).
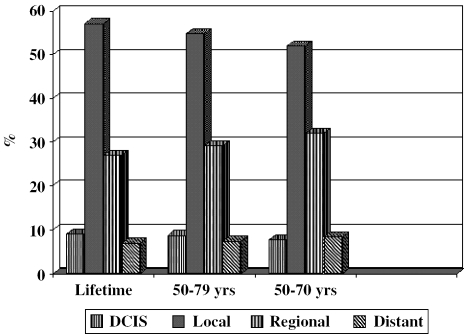
Design and population: We used a stochastic model with proxies of age-dependent biology to evaluate the incremental U.S. societal costs and benefits of biennial screening from age 50 until age 70, 79, or lifetime.
Main outcome measures: Discounted incremental costs per life years saved (LYS).
Results: Lifetime screening is expensive (151,434 dollars per LYS) if women have treatment and survival comparable to clinical trials (idealized); stopping at age 79 costs 82,063 dollars per LYS. This latter result corresponds to costs associated with an LE of 9.5 years at age 79, a value expected for 75% of 79-year-olds, about 50% of 80-year-olds, and 25% of 85-year-olds. Using actual treatment and survival patterns, screening benefits are greater, and lifetime screening of all women might be considered (114,905 dollars per LYS), especially for women in the top 25% of LE for their age (50,643 dollars per LYS, life expectancy of approximately 7 years at age 90).
Conclusions: If all women receive idealized treatment, the benefits of mammography beyond age 79 are too low relative to their costs to justify continued screening. However, if treatment is not ideal, extending screening beyond age 79 could be considered, especially for women in the top 25% of life expectancy for their age.
Figures
Comment in
-
The use of life expectancy in cancer screening guidelines. Moving with caution from model-based evidence to evidence-based guidelines.J Gen Intern Med. 2005 Jun;20(6):552-3. doi: 10.1111/j.1525-1497.2005.41012.x. J Gen Intern Med. 2005. PMID: 15987335 Free PMC article. No abstract available.
References
-
- Ershler WB, Longo DL. Aging and cancer. issues of basic and clinical science J Natl Cancer Inst. 1997;89:1489–1497. - PubMed
-
- Ries LAG, Kosary CL, Hankey BF, Edwards BK. SEER Cancer Statistic Review, 1973–1996. DHHS, NIH, NCI, Bethesda, MD:1999.
-
- U.S. Bureau of the Census. Current Population Survey, July 2002. Available at:
-
- Soldo BJ, Agree EM. America's Elderly. Washington, DC: Population Reference Bureau, Inc.; 1988. - PubMed
-
- Lash TL, Silliman RA. Prevalence of cancer. J Natl Cancer Inst. 1998;90:399–400. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical