

Effect of ventilator-associated tracheobronchitis on outcome in patients without chronic respiratory failure: a case-control study
- PMID: 15987396
- PMCID: PMC1175884
- DOI: 10.1186/cc3508
Effect of ventilator-associated tracheobronchitis on outcome in patients without chronic respiratory failure: a case-control study
Abstract
Introduction: Our objective was to determine the effect of ventilator-associated tracheobronchitis (VAT) on outcome in patients without chronic respiratory failure.
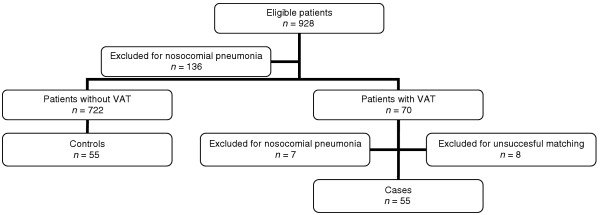
Methods: This was a retrospective observational matched study, conducted in a 30-bed intensive care unit (ICU). All immunocompetent, nontrauma, ventilated patients without chronic respiratory failure admitted over a 6.5-year period were included. Data were collected prospectively. Patients with nosocomial pneumonia, either before or after VAT, were excluded. Only first episodes of VAT occurring more than 48 hours after initiation of mechanical ventilation were studied. Six criteria were used to match cases with controls, including duration of mechanical ventilation before VAT. Cases were compared with controls using McNemar's test and Wilcoxon signed-rank test for qualitative and quantitative variables, respectively. Variables associated with a duration of mechanical ventilation longer than median were identified using univariate and multivariate analyses.
Results: Using the six criteria, it was possible to match 55 (87%) of the VAT patients (cases) with non-VAT patients (controls). Pseudomonas aeruginosa was the most frequently isolated bacteria (34%). Although mortality rates were similar between cases and controls (29% versus 36%; P = 0.29), the median duration of mechanical ventilation (17 days [range 3-95 days] versus 8 [3-61 days]; P < 0.001) and ICU stay (24 days [range 5-95 days] versus 12 [4-74] days; P < 0.001) were longer in cases than in controls. Renal failure (odds ratio [OR] = 4.9, 95% confidence interval [CI] = 1.6-14.6; P = 0.004), tracheostomy (OR = 4, 95% CI = 1.1-14.5; P = 0.032), and VAT (OR = 3.5, 95% CI = 1.5-8.3; P = 0.004) were independently associated with duration of mechanical ventilation longer than median.
Conclusion: VAT is associated with longer durations of mechanical ventilation and ICU stay in patients not suffering from chronic respiratory failure.
Figures
Comment in
-
Does ventilator-associated tracheobronchitis need antibiotic treatment?Crit Care. 2005 Jun;9(3):255-6. doi: 10.1186/cc3535. Epub 2005 May 3. Crit Care. 2005. PMID: 15987416 Free PMC article.
References
-
- Vincent JL, Bihari DJ, Suter PM, Bruining HA, White J, Nicolas-Chanoin MH, Wolff M, Spencer RC, Hemmer M. The prevalence of nosocomial infection in intensive care units in Europe. Results of the European Prevalence of Infection in Intensive Care (EPIC) Study. EPIC International Advisory Committee. JAMA. 1995;274:639–644. doi: 10.1001/jama.274.8.639. - DOI - PubMed
-
- Rello J, Ausina V, Castella J, Net A, Prats G. Nosocomial respiratory tract infections in multiple trauma patients. Influence of level of consciousness with implications for therapy. Chest. 1992;102:525–529. - PubMed
-
- Nseir S, Di Pompeo C, Pronnier P, Beague S, Onimus T, Saulnier F, Grandbastien B, Mathieu D, Delvallez-Roussel M, Durocher A. Nosocomial tracheobronchitis in mechanically ventilated patients: incidence, aetiology and outcome. Eur Respir J. 2002;20:1483–1489. doi: 10.1183/09031936.02.00012902. - DOI - PubMed
-
- Marquette CH, Georges H, Wallet F, Ramon P, Saulnier F, Neviere R, Mathieu D, Rime A, Tonnel AB. Diagnostic efficiency of endotracheal aspirates with quantitative bacterial cultures in intubated patients with suspected pneumonia. Comparison with the protected specimen brush. Am Rev Respir Dis. 1993;148:138–144. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
