

Acute phase reactants add little to composite disease activity indices for rheumatoid arthritis: validation of a clinical activity score
- PMID: 15987481
- PMCID: PMC1175030
- DOI: 10.1186/ar1740
Acute phase reactants add little to composite disease activity indices for rheumatoid arthritis: validation of a clinical activity score
Abstract
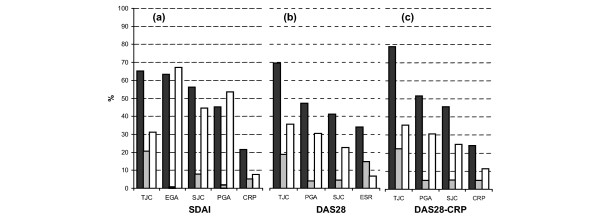
Introduction: Frequent assessments of rheumatoid arthritis (RA) disease activity allow timely adaptation of therapy, which is essential in preventing disease progression. However, values of acute phase reactants (APRs) are needed to calculate current composite activity indices, such as the Disease Activity Score (DAS)28, the DAS28-CRP (i.e. the DAS28 using C-reactive protein instead of erythrocyte sedimentation rate) and the Simplified Disease Activity Index (SDAI). We hypothesized that APRs make limited contribution to the SDAI, and that an SDAI-modification eliminating APRs - termed the Clinical Disease Activity Index (CDAI; i.e. the sum of tender and swollen joint counts [28 joints] and patient and physician global assessments [in cm]) - would have comparable validity in clinical cohorts.
Method: Data sources comprised an observational cohort of 767 RA patients (average disease duration 8.1 +/- 10.6 years), and an independent inception cohort of 106 patients (disease duration 11.5 +/- 12.5 weeks) who were followed prospectively.
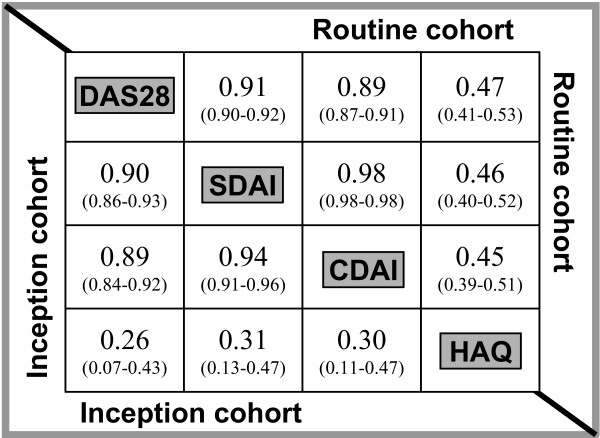
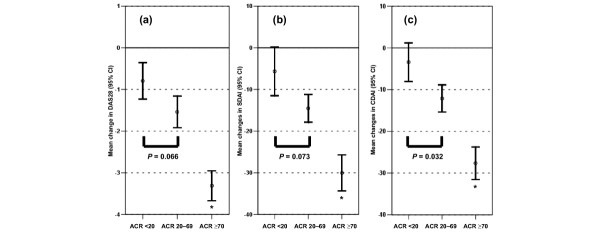
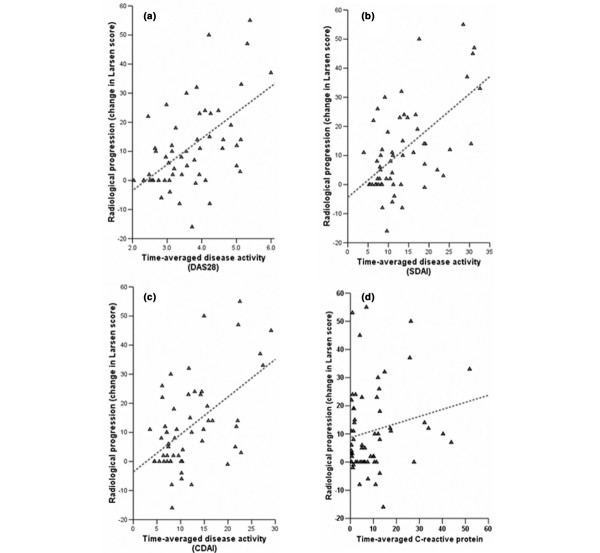
Results: Our clinically based hypothesis was statistically supported: APRs accounted only for 15% of the DAS28, and for 5% of the SDAI and the DAS28-CRP. In both cohorts the CDAI correlated strongly with DAS28 (R = 0.89-0.90) and comparably to the correlation of SDAI with DAS28 (R = 0.90-0.91). In additional analyses, the CDAI when compared to the SDAI and the DAS28 agreed with a weighted kappa of 0.70 and 0.79, respectively, and comparably to the agreement between DAS28 and DAS28-CRP. All three scores correlated similarly with Health Assessment Questionnaire (HAQ) scores (R = 0.45-0.47). The average changes in all scores were greater in patients with better American College of Rheumatology response (P < 0.0001, analysis of variance; discriminant validity). All scores exhibited similar correlations with radiological progression (construct validity) over 3 years (R = 0.54-0.58; P < 0.0001).
Conclusion: APRs add little information on top (and independent) of the combination of clinical variables included in the SDAI. A purely clinical score is a valid measure of disease activity and will have its greatest merits in clinical practice rather than research, where APRs are usually always available. The CDAI may facilitate immediate and consistent treatment decisions and help to improve patient outcomes in the longer term.
Figures
References
-
- Plant MJ, Williams AL, O'Sullivan MM, Lewis PA, Coles EC, Jessop JD. Relationship between time-integrated C-reactive protein levels and radiologic progression in patients with rheumatoid arthritis. Arthritis Rheum. 2000;43:1473–1477. doi: 10.1002/1529-0131(200007)43:7<1473::AID-ANR9>3.0.CO;2-N. - DOI - PubMed
-
- Welsing PM, Landewe RB, van Riel PL, Boers M, van Gestel AM, van der Linden S, Swinkels HL, van der Heijde DM. The relationship between disease activity and radiologic progression in patients with rheumatoid arthritis: a longitudinal analysis. Arthritis Rheum. 2004:2082–2093. doi: 10.1002/art.20350. - DOI - PubMed
-
- Fuchs HA, Kaye JJ, Callahan LF, Nance EP, Pincus T. Evidence of significant radiographic damage in rheumatoid arthritis within the first 2 years of disease. J Rheumatol. 1989;16:585–591. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
