Fine-needle aspiration of the thyroid: an overview
- PMID: 15987502
- PMCID: PMC1184092
- DOI: 10.1186/1742-6413-2-12
Fine-needle aspiration of the thyroid: an overview
Abstract
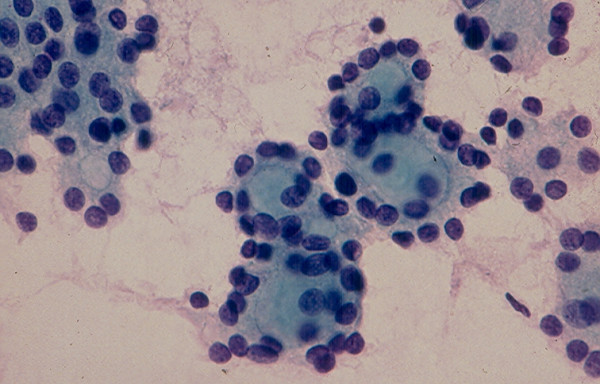
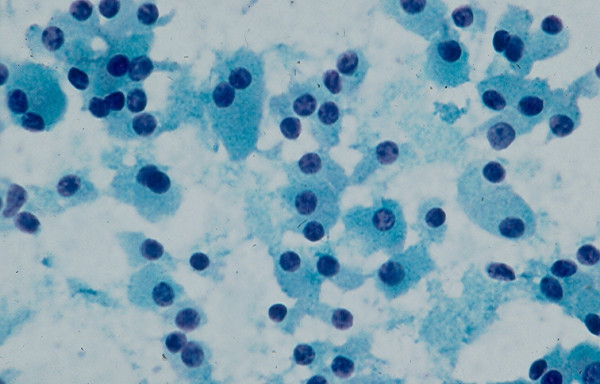
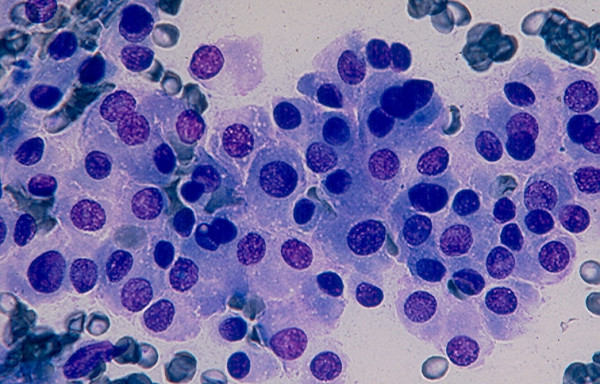
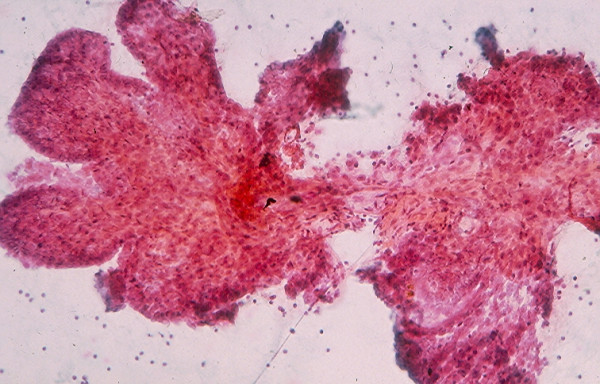
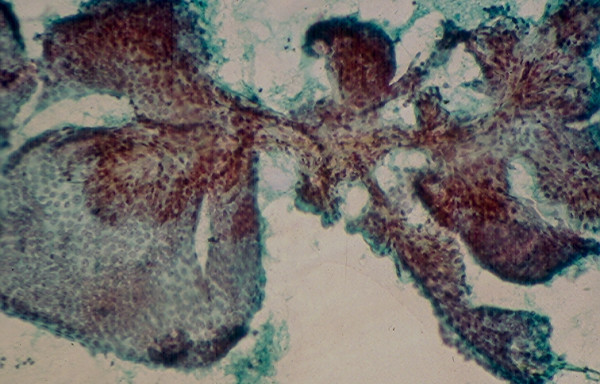
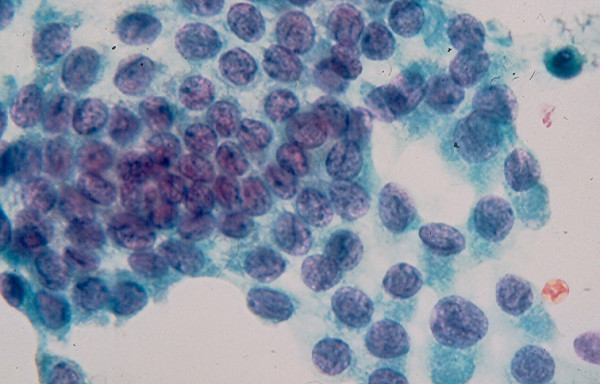
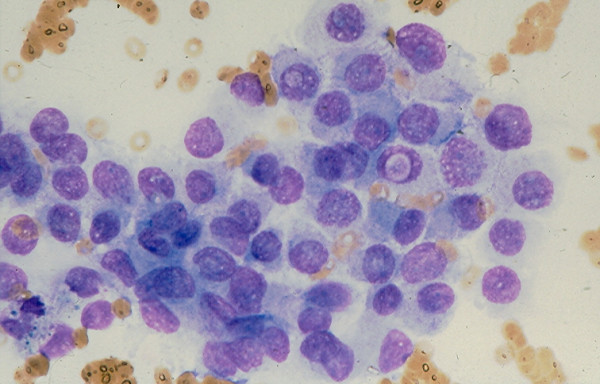
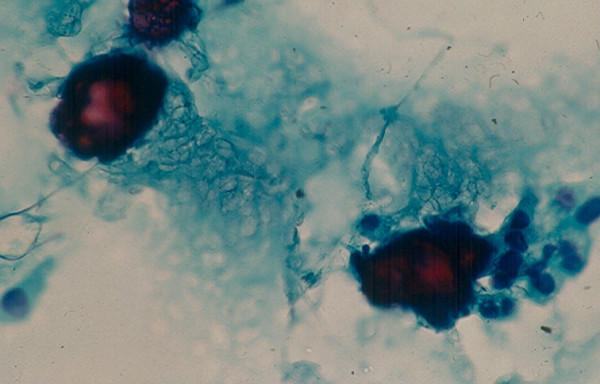
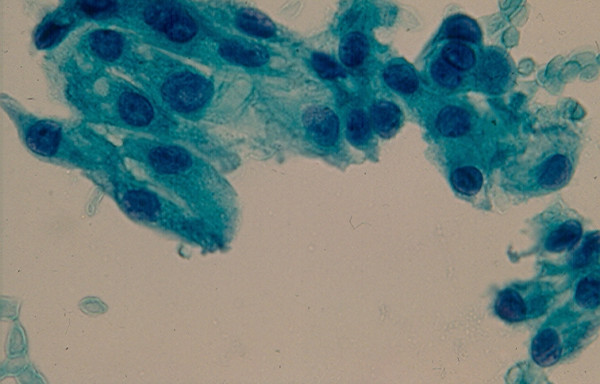
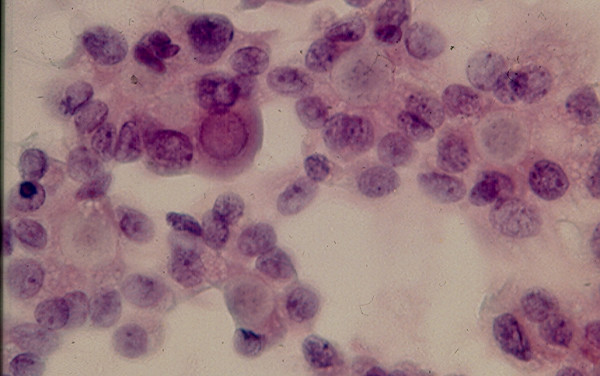
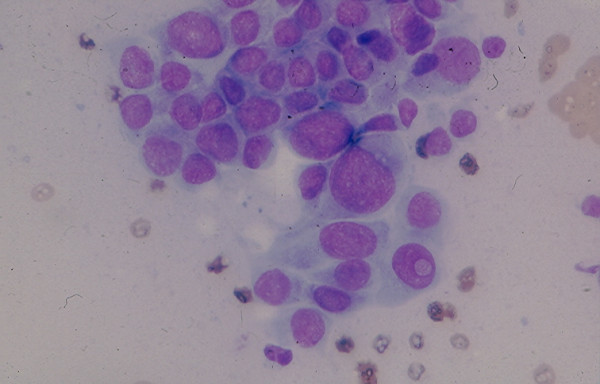
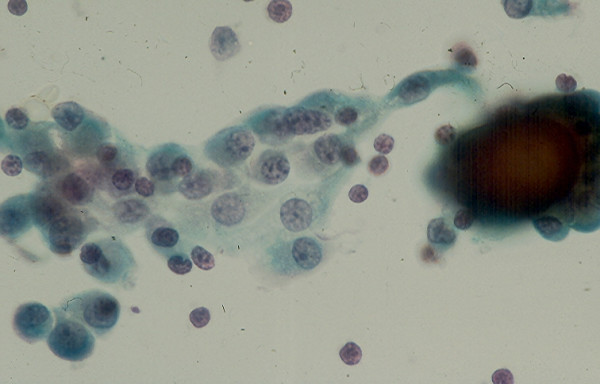
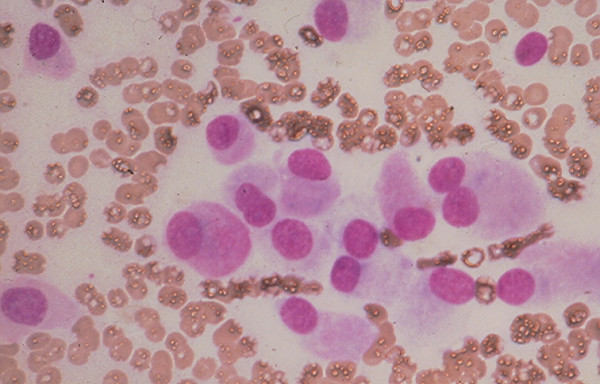
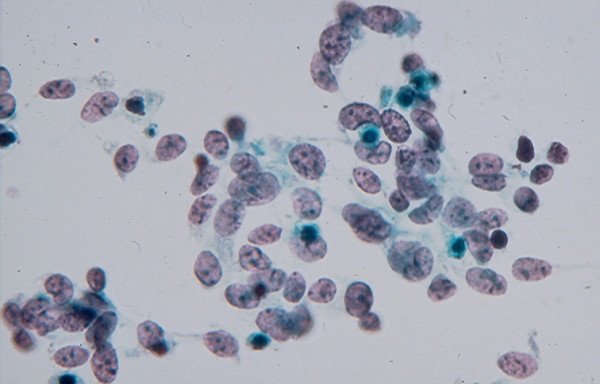
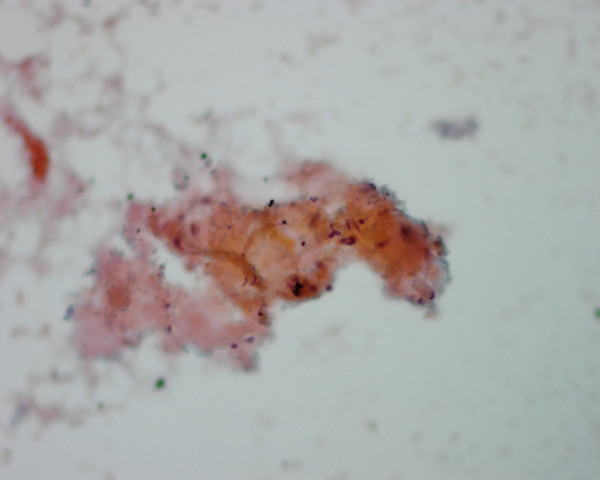
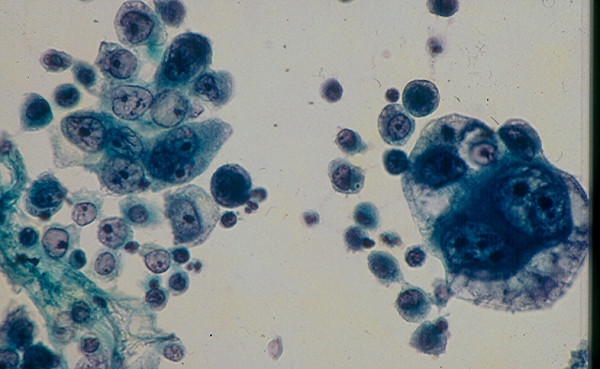
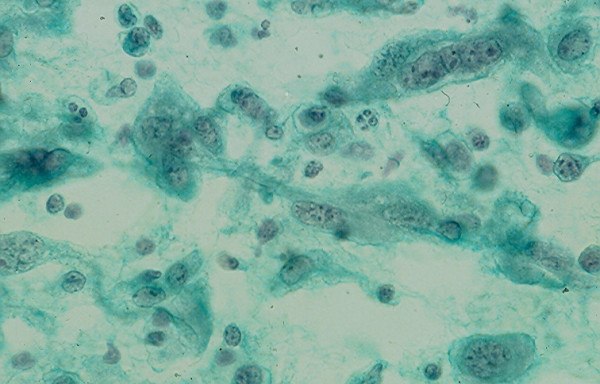
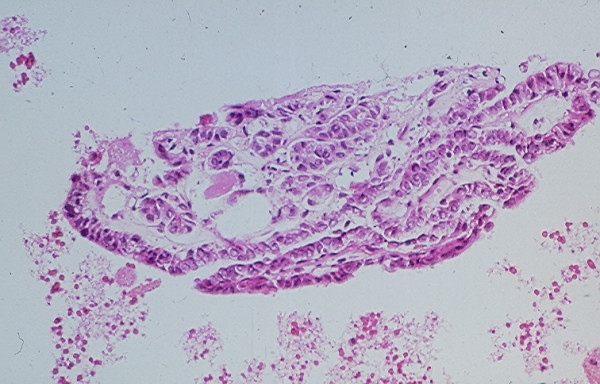
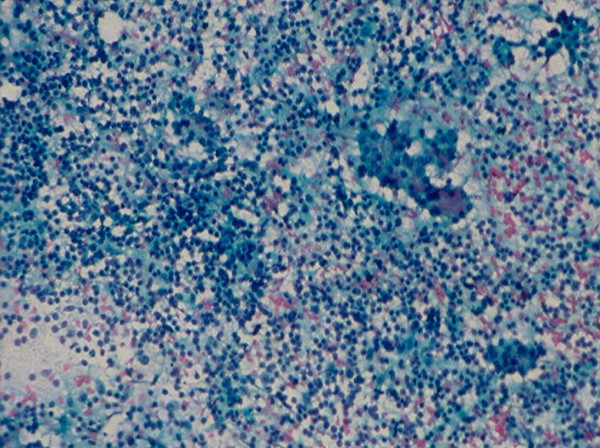
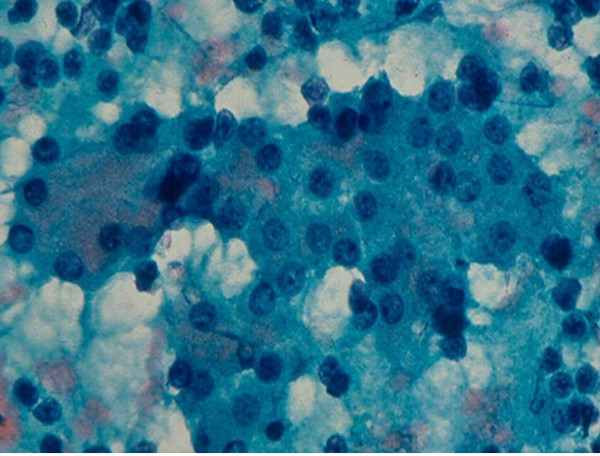
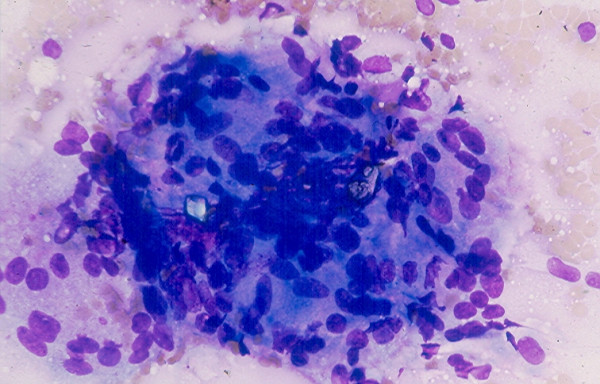
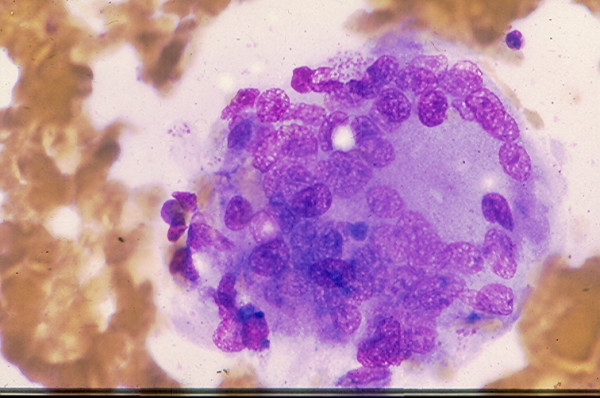
Thyroid nodules (TN) are a common clinical problem. Fine needle aspiration (FNA) of the thyroid now is practiced worldwide and proves to be the most economical and reliable diagnostic procedure to identify TNs that need surgical excision and TNs that can be managed conservatively. The key for the success of thyroid FNA consists of an adequate or representative cell sample and the expertise in thyroid cytology. The FNA cytologic manifestations of TNs may be classified into seven working cytodiagnostic groups consisting of a few heterogenous lesions each to facilitate the differential diagnosis. Recent application of diagnostic molecular techniques to aspirated thyroid cells proved to be useful in separating benign from malignant TNs in several cases of indeterminate lesions.
Figures


References
-
- Frazell EL, Foote FW. Papillary carcinoma of the thyroid: a review of 25 years of experience. Cancer. 1958;11:895–922. - PubMed
-
- Soderstrom N. Puncture of goiters for aspiration biopsy. A primary report. Acta Med Scand. 1952;144:237–244. - PubMed
-
- Eihorn J, Franzen S. Thin needle biopsy in the diagnosis of thyroid disease. Acta Radiol. 1962;58:321–336.
LinkOut - more resources
Full Text Sources
Other Literature Sources