

How strong is the evidence for the use of perioperative beta blockers in non-cardiac surgery? Systematic review and meta-analysis of randomised controlled trials
- PMID: 15996966
- PMCID: PMC1183126
- DOI: 10.1136/bmj.38503.623646.8F
How strong is the evidence for the use of perioperative beta blockers in non-cardiac surgery? Systematic review and meta-analysis of randomised controlled trials
Abstract
Objective: To determine the effect of perioperative beta blocker treatment in patients having non-cardiac surgery.
Design: Systematic review and meta-analysis.
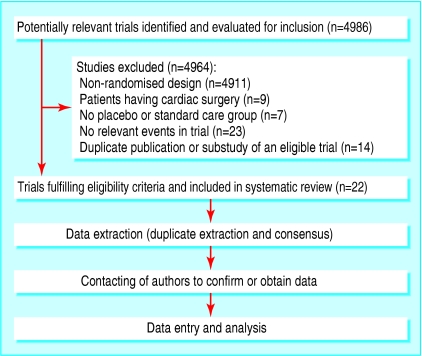
Data sources: Seven search strategies, including searching two bibliographic databases and hand searching seven medical journals. STUDY SELECTION AND OUTCOMES: We included randomised controlled trials that evaluated beta blocker treatment in patients having non-cardiac surgery. Perioperative outcomes within 30 days of surgery included total mortality, cardiovascular mortality, non-fatal myocardial infarction, non-fatal cardiac arrest, non-fatal stroke, congestive heart failure, hypotension needing treatment, bradycardia needing treatment, and bronchospasm.
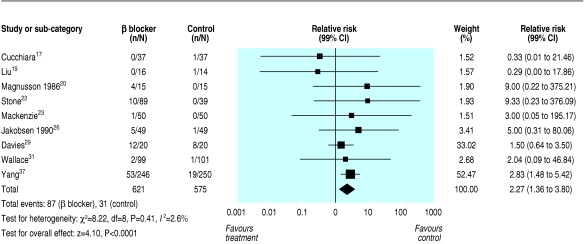
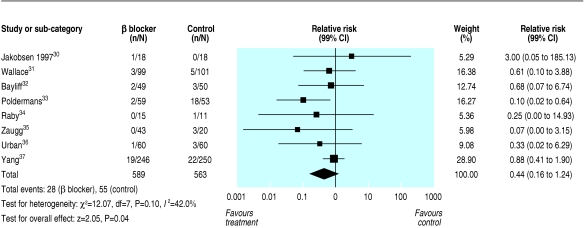
Results: Twenty two trials that randomised a total of 2437 patients met the eligibility criteria. Perioperative beta blockers did not show any statistically significant beneficial effects on any of the individual outcomes and the only nominally statistically significant beneficial relative risk was 0.44 (95% confidence interval 0.20 to 0.97, 99% confidence interval 0.16 to 1.24) for the composite outcome of cardiovascular mortality, non-fatal myocardial infarction, and non-fatal cardiac arrest. Methods adapted from formal interim monitoring boundaries applied to cumulative meta-analysis showed that the evidence failed, by a considerable degree, to meet standards for forgoing additional studies. The individual safety outcomes in patients treated with perioperative beta blockers showed a relative risk for bradycardia needing treatment of 2.27 (95% CI 1.53 to 3.36, 99% CI 1.36 to 3.80) and a nominally statistically significant relative risk for hypotension needing treatment of 1.27 (95% CI 1.04 to 1.56, 99% CI 0.97 to 1.66).
Conclusion: The evidence that perioperative beta blockers reduce major cardiovascular events is encouraging but too unreliable to allow definitive conclusions to be drawn.
Figures

Comment in
-
Beta blockers for patients at risk of cardiac events during non-cardiac surgery.BMJ. 2005 Oct 22;331(7522):919-20. doi: 10.1136/bmj.331.7522.919. BMJ. 2005. PMID: 16239671 Free PMC article. No abstract available.
-
Review: evidence of benefit for perioperative beta-blockers in noncardiac surgery is unreliable.ACP J Club. 2006 Jan-Feb;144(1):17. ACP J Club. 2006. PMID: 16388566 No abstract available.
References
-
- Sametz W, Metzler H, Gries M, Porta S, Sadjak A, Supanz S, et al. Perioperative catecholamine changes in cardiac risk patients. Eur J Clin Invest 1999;29: 582-7. - PubMed
-
- Parker SD, Breslow MJ, Frank SM, Rosenfeld BA, Norris EJ, Christopherson R, et al. Catecholamine and cortisol responses to lower extremity revascularization: correlation with outcome variables. Crit Care Med 1995;23: 1954-61. - PubMed
-
- Priebe HJ. Triggers of perioperative myocardial ischaemia and infarction. Br J Anaesth 2004;93: 9-20. - PubMed
-
- Weissman C. The metabolic response to stress: an overview and update. Anesthesiology 1990;73: 308-27. - PubMed
-
- Lee TH. Reducing cardiac risk in noncardiac surgery. N Engl J Med 1999;341: 1838-40. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous