

Gorham's disease or massive osteolysis
- PMID: 16012123
- PMCID: PMC1183435
- DOI: 10.3121/cmr.3.2.65
Gorham's disease or massive osteolysis
Abstract
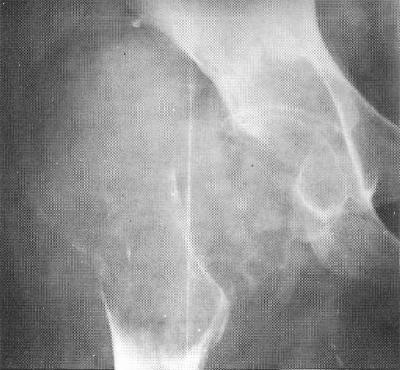
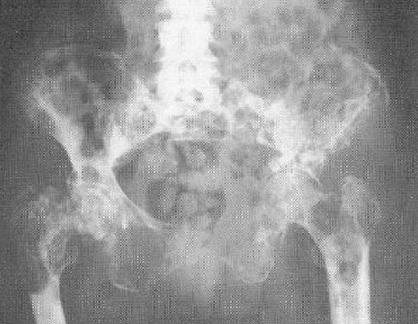
Gorham's disease is a rare disorder characterized by proliferation of vascular channels that results in destruction and resorption of osseous matrix. Since the initial description of the disease by Gorham and colleagues (1954) and by Gorham and Stout (1955), fifty years have elapsed but still the precise etiology of Gorham's disease remains poorly understood and largely unknown. There is no evidence of a malignant, neuropathic, or infectious component involved in the causation of this disorder. The mechanism of bone resorption is unclear. The clinical presentation of Gorham's disease is variable and depends on the site of involvement. It often takes many months or years before the offending lesion is correctly diagnosed. A high index of clinical suspicion is needed to arrive at an early, accurate diagnosis. Patients with Gorham's disease may complain of dull aching pain or insidious onset of progressive weakness. In some cases, pathologic fracture often leads to its discovery. Gorham's disease is progressive in most patients; however, in some cases, the disease process is self-limiting. The clinical course is generally protracted but rarely fatal, with eventual stabilization of the affected bone being the most common sequelae. Chylous pericardial and pleural effusions may occur due to mediastinal extension of the disease process from the involved vertebra, scapula, rib or sternum, and can be life threatening. A high morbidity and mortality is seen in patients with spinal and/or visceral involvement. The medical treatment for Gorham's disease includes radiation therapy, anti-osteoclastic medications (bisphosphonates), and alpha-2b interferon. Surgical treatment options include resection of the lesion and reconstruction using bone grafts and/or prostheses. In most cases, bone grafts tend to undergo resorption and are not helpful. Surgical reconstruction and/or radiation therapy are used for management of patients who have large, symptomatic lesions with long-standing, disabling functional instability. Surgical stabilization may be required for unstable spinal lesions. Various treatment options, including pleurectomy, pleurodesis, thoracic duct ligation, radiation therapy, interferon therapy, and bleomycin, have been used for management of patients with Gorham's disease presenting with chylothorax. In general, no single treatment modality has proven effective in arresting the disease.
Figures



Comment on
-
A case of Gorham's disease with chylothorax treated curatively with radiation therapy.Clin Med Res. 2005 May;3(2):83-6. doi: 10.3121/cmr.3.2.83. Clin Med Res. 2005. PMID: 16012125 Free PMC article.
References
-
- Gorham LW, Wright AW, Shultz HH, Maxon FC, Jr. Disappearing bones: a rare form of massive osteolysis: report of two cases, one with autopsy findings. Am J Med 1954;17:674–682. - PubMed
-
- Gorham LW, Stout AP. Massive osteolysis (acute spontaneous absorption of bone, phantom bone, disappearing bone): its relation to hemangiomatosis. J Bone Joint Surg [Am] 1955;37-A:985–1004. - PubMed
-
- Hambach R, Pujman J, Maly V. Massive osteolysis due to hemangiomatosis: report of a case of Gorham’s disease with autopsy. Radiology 1958;71:43–47. - PubMed
-
- Halliday DR, Dahlin DC, Pugh DG, Young HH. Massive osteolysis and angiomatosis. Radiology 1964;82:637–644. - PubMed
-
- Poirier H. Massive osteolysis of the humerus treated by resection and prosthetic replacement. J Bone Joint Surg [Br] 1968;50-B:158–160. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources