

Accuracy of noninvasive ejection fraction measurement in a large community-based clinic
- PMID: 16012124
- PMCID: PMC1183436
- DOI: 10.3121/cmr.3.2.75
Accuracy of noninvasive ejection fraction measurement in a large community-based clinic
Abstract
Objective: Compare the agreement of two dimensional echocardiography (echocardiography) and electrocardiogram (ECG)-gated single photon emission computed tomography (SPECT), with left ventricular contrast angiography (angiography) for the evaluation of left ventricular ejection fraction (LVEF).
Design: Retrospective cohort study.
Data source: American College of Cardiology National Cardiovascular Data Registry(TM) (ACC-NCDR).
Participants: Patients from a large, community-based clinic in central Wisconsin.
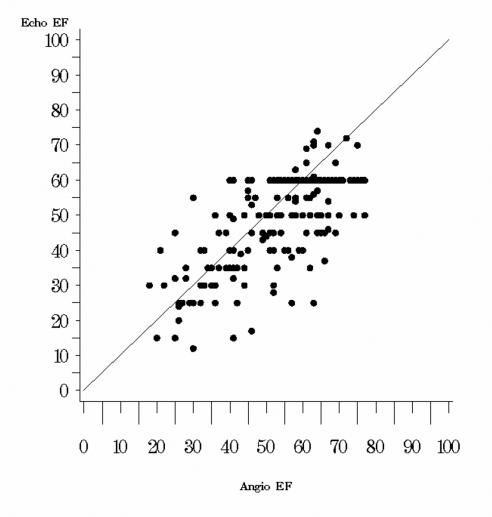
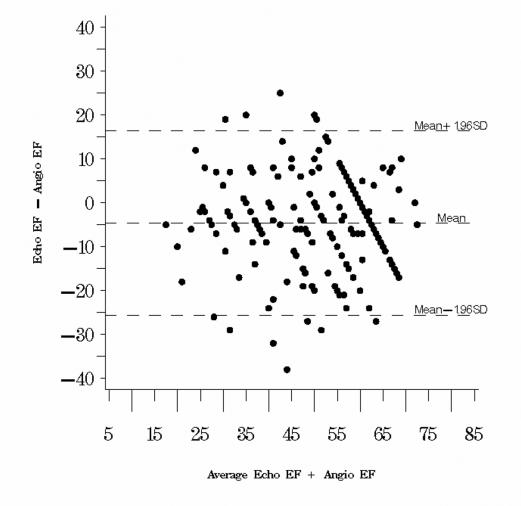
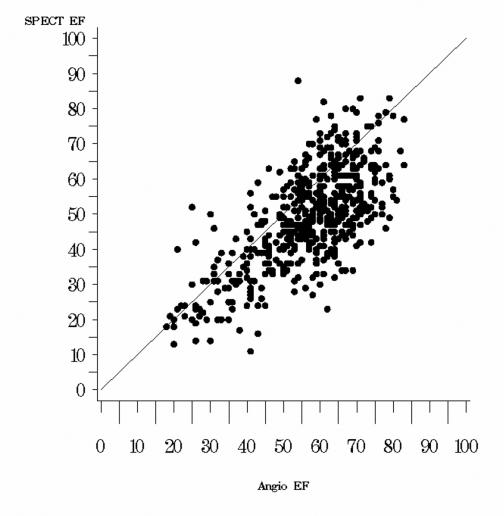
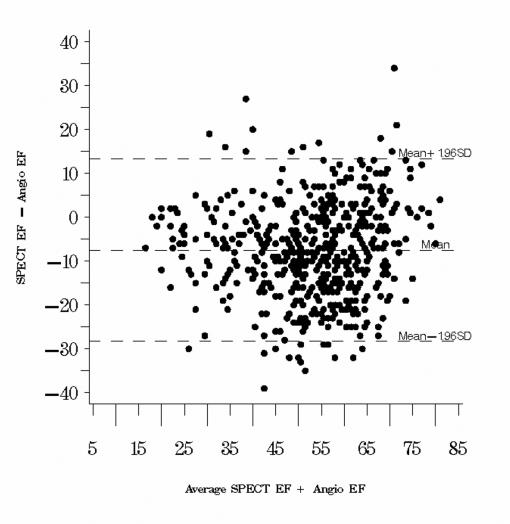
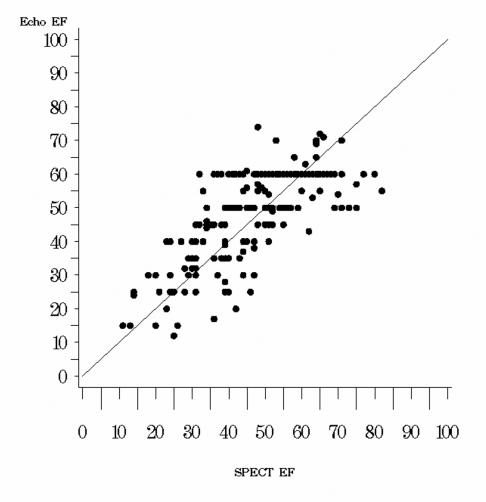
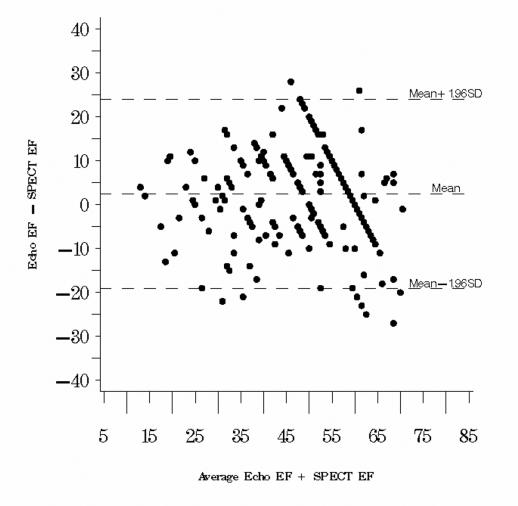
Methods: Consecutive patients (1999-2002) were identified from the ACC-NCDR dataset who underwent angiography and echocardiography or SPECT within 1 month of each other for evaluation of LVEF. Noninvasive LVEF values were compared to those obtained by angiography using the paired t-test. Regression analysis was used to assess the relation between the compared methods. Bland-Altman analyses were performed to assess the agreement between LVEF values obtained by the noninvasive techniques and angiography. Sensitivity and specificity of detecting depressed LVEF were determined for noninvasive techniques. Regression equations were determined for estimating angiographic values from the echocardiographic or SPECT values.
Results: Five hundred thirty-four patients underwent 542 angiographic studies: SPECT in all 534 patients, combined SPECT and echocardiographic studies in 201 patients, and combined angiographic and echocardiographic studies in 202 patients. Correlation of angiographic LVEFs with both echocardiographic and SPECT LVEFs was significant (r = 0.70 and r = 0.69, respectively; p < 0.0001). Echocardiographic LVEFs were lower than those determined by angiography (49% +/- 1.0% versus 54% +/- 1.0%; p < 0.0001). SPECT LVEFs were also lower than angiographic LVEFs (49% +/- 0.6% versus 57% +/- 0.6%; p < 0.0001). For 201 patients who underwent both SPECT and echocardiography, SPECT LVEFs were lower (47% +/- 1.0% for SPECT versus 49% +/- 1.0% for echocardiography; p < 0.05). Bland-Altman analysis revealed widely varying differences between techniques with broad confidence intervals. Nonetheless, sensitivity and specificity for determining LVEFs of <40% for SPECT and echocardiography were 90% and 86%, and 75% and 89%, respectively. LVEF of < or = 35% was correctly assessed by both SPECT and echocardiography. Sensitivity and specificity for SPECT were 82% and 89%, and 81% and 88% for echocardiography.
Conclusion: At our institution, LVEFs obtained noninvasively by echocardiography or SPECT are lower than angiographic LVEFs with widely fluctuating differences. Regression equations can be used to correct the noninvasive readings. Although lower, noninvasive techniques appear to accurately assess depressed LVEFs (<40% and <35%). The accuracy of noninvasive techniques for the evaluation of LVEF should be considered when managing and determining prognoses of patients with cardiac conditions. Individual institutions should determine the validity of the noninvasive techniques they use to assess LVEF.
Figures
Comment in
-
Ejection fraction derived by noninvasive modalities versus left ventricular angiographic determination.Clin Med Res. 2005 May;3(2):61-2. doi: 10.3121/cmr.3.2.61. Clin Med Res. 2005. PMID: 16012121 Free PMC article. No abstract available.
Similar articles
-
Assessment of ejection fraction with Tl-201 gated SPECT in myocardial infarction: Precision in a rest-redistribution study and accuracy versus planar angiography.J Nucl Cardiol. 2001 Jan-Feb;8(1):31-9. doi: 10.1067/mnc.2001.109863. J Nucl Cardiol. 2001. PMID: 11182707
-
Gated 99mTc-MIBI single-photon emission computed tomography for the evaluation of left ventricular ejection fraction: comparison with three-dimensional echocardiography.Ann Nucl Med. 2008 Oct;22(8):723-6. doi: 10.1007/s12149-008-0165-9. Epub 2008 Nov 4. Ann Nucl Med. 2008. PMID: 18982477
-
Comparison of LVEF assessed by 2D echocardiography, gated blood pool SPECT, 99mTc tetrofosmin gated SPECT, and 18F-FDG gated PET with ERNV in patients with CAD and severe LV dysfunction.Nucl Med Commun. 2014 Nov;35(11):1156-61. doi: 10.1097/MNM.0000000000000182. Nucl Med Commun. 2014. PMID: 25144559 Clinical Trial.
-
[Role of perfusion myocardial scintigraphy with gated SPECT technique in the diagnostic and prognostic evaluation of patients with chronic coronary disease].Ital Heart J Suppl. 2002 Mar;3(3):309-18. Ital Heart J Suppl. 2002. PMID: 12040846 Review. Italian.
-
European Association of Cardiovascular Imaging/Cardiovascular Imaging Department of the Brazilian Society of Cardiology recommendations for the use of cardiac imaging to assess and follow patients after heart transplantation.Eur Heart J Cardiovasc Imaging. 2015 Sep;16(9):919-48. doi: 10.1093/ehjci/jev139. Epub 2015 Jul 2. Eur Heart J Cardiovasc Imaging. 2015. PMID: 26139361 Review.
Cited by
-
Cost-effectiveness of the children's oncology group long-term follow-up screening guidelines for childhood cancer survivors at risk for treatment-related heart failure.Ann Intern Med. 2014 May 20;160(10):672-83. doi: 10.7326/M13-2498. Ann Intern Med. 2014. PMID: 24842414 Free PMC article.
-
The role of imaging in the management of cardiorenal syndrome.Int J Nephrol. 2011 Jan 24;2011:245241. doi: 10.4061/2011/245241. Int J Nephrol. 2011. PMID: 21318046 Free PMC article.
-
Contractility evaluation by 2 dimensional echocardiography and gated SPECT myocardial perfusion scintigraphy in hypertensive patients with clinical presentation of atypical chest pain.Hippokratia. 2011 Jan;15(1):64-8. Hippokratia. 2011. PMID: 21607039 Free PMC article.
-
Comparison of left ventricular ejection fraction values obtained using invasive contrast left ventriculography, two-dimensional echocardiography, and gated single-photon emission computed tomography.SAGE Open Med. 2016 Jun 24;4:2050312116655940. doi: 10.1177/2050312116655940. eCollection 2016. SAGE Open Med. 2016. PMID: 27621804 Free PMC article.
-
Left ventricular ejection fraction assessment by Tl-201 gated SPECT: a comparison with echocardiography.Clin Cardiol. 2010 Mar;33(3):E56-62. doi: 10.1002/clc.20577. Clin Cardiol. 2010. PMID: 20127905 Free PMC article.
References
-
- Grimm W, Glaveris C, Hoffmann J, Mena V, Mey N, Born S, Maisch B. Noninvasive arrhythmia risk stratification in idiopathic dilated cardiomyopathy: design and first results of the Marburg Cardiomyopathy Study. Pacing Clin Electrophysiol 1998;21:2551–2556. - PubMed
-
- Grimm W, Christ M, Bach J, Muller HH, Maisch B. Noninvasive arrhythmia risk stratification in idiopathic dilated cardiomyopathy: results of the Marburg Cardiomyopathy Study. Circulation 2003;108:2883–2891. - PubMed
-
- Klein H, Auricchio A, Reek S, Geller C. New primary prevention trials of sudden cardiac death in patients with left ventricular dysfunction: SCD-HEFT and MADIT-II. Am J Cardiol 1999;83:91D–97D. - PubMed
-
- Theal M, Demers C, Mckelvie RS. The role of angiotensin II receptor blockers in the treatment of heart failure patients. Congest Heart Fail 2003;9:29–34. - PubMed
-
- Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R, Feigenbaum H, Gutgesell H, Reichek N, Sahn D, Schnittger I, et al. Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. American Society of Echocardiography Committee on Standards, Subcommittee on Quantitation of Two-Dimensional Echocardiograms. J Am Soc Echocardiogr 1989;2:358–367. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical