

Effectiveness of repeated video feedback in the acquisition of a surgical technical skill
- PMID: 16013622
- PMCID: PMC3211542
Effectiveness of repeated video feedback in the acquisition of a surgical technical skill
Abstract
Background: Previously we evaluated the effectiveness of videotaped feedback as a teaching tool for surgical residents using 3 different core skills in the field of orthopedics. Our results revealed no significant differences in technical skill among surgical residents who were exposed to videotaped feedback and those who were not. Several limitations in the study were identified, including the presence of only a single exposure to videotaped feedback. In the present study we included repeated exposures to determine if skill acquisition was enhanced.
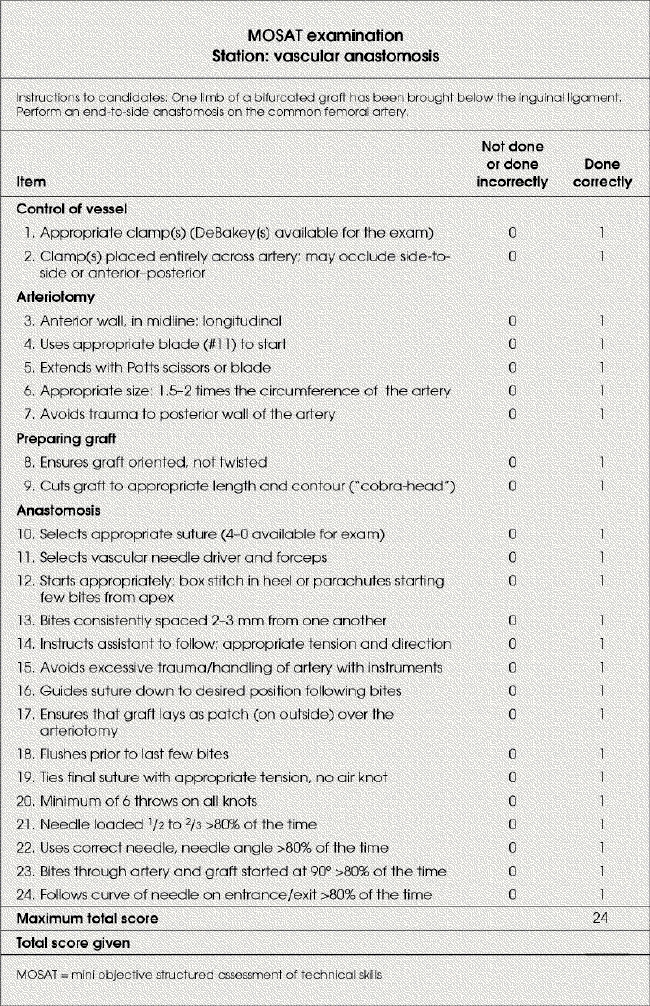
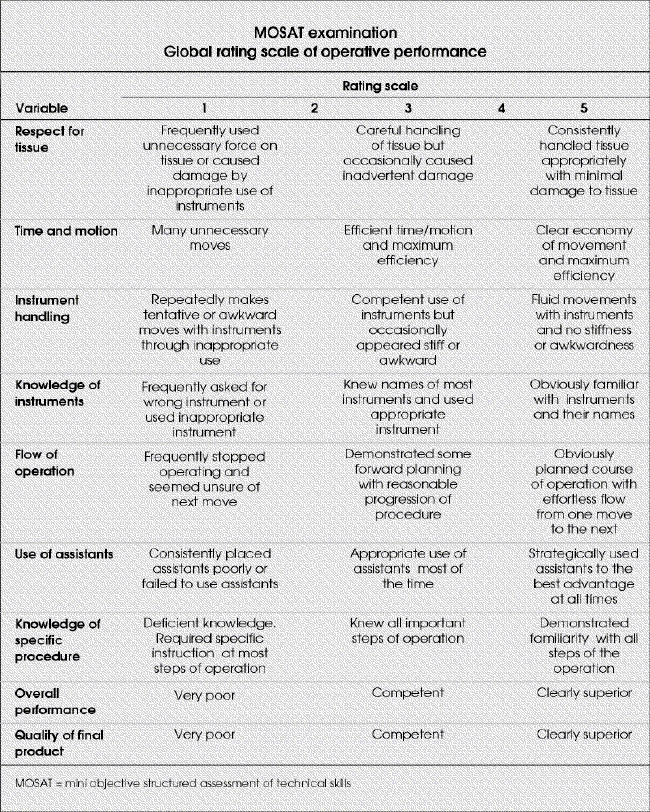
Methods: Thirty-three surgical residents were randomly assigned to receive either no videotaped feedback (control group) or repeated video feedback over 3 consecutive weekly practice sessions on a vascular anastomosis bench model. On the fourth week, vascular surgeons blinded to the 2 groups evaluated the residents on the same vascular anastomosis task using a global rating scale and technical checklist forms.
Results: Twenty-six (79%) of the residents participated. Independent t tests comparing the scores of each of the 2 different measures between the control group and repeated videotaped feedback group revealed no statistically significant differences.
Conclusions: There was no significant difference in the performance of a vascular anastomosis in a bench-training model between residents who were exposed to video feedback over several practice sessions and those who received no video feedback.
Contexte: Nous avions évalué auparavant l'efficacité des commentaires enregistrés sur bande vidéo comme outil de formation des résidents en chirurgie en utilisant trois différentes compétences de base en orthopédie. Nos résultats n'ont révélé aucune différence importante au niveau des compétences techniques chez les résidents en chirurgie exposés aux commentaires vidéo par rapport à ceux qui ne l'ont pas été. On a déterminé plusieurs limites de l'étude, y compris la présence d'une seule exposition aux commentaires vidéo. Dans la présente étude, nous avons inclus des expositions répétées afin de déterminer si elles amélioraient l'acquisition de compétences.
Méthodes: On a réparti au hasard 33 résidents en chirurgie en groupes qui ne recevraient aucun commentaire vidéo (groupe témoin) ou recevraient des commentaires vidéo répétés pendant trois séances de pratique hebdomadaire consécutives sur un banc d'essai d'anastomose vasculaire. Au cours de la quatrième semaine, des chirurgiens vasculaires ne connaissant pas la répartition des deux groupes ont utilisé une échelle d'évaluation globale et des formulaires de contrôle technique pour évaluer les résidents qui ont pratiqué la même intervention d'anastomose vasculaire.
Résultats: Vingt-six (79 %) des résidents ont participé. Des tests t indépendants comparant les résultats de chacune des deux mesures différentes entre le groupe témoin et celui des sujets exposés à des commentaires vidéo répétés n'ont révélé aucune différence statistiquement significative.
Conclusions: Il n'y avait pas de différence significative au niveau de l'exécution d'une anastomose vasculaire dans un modèle sur banc d'essai entre les résidents exposés à des commentaires vidéo pendant plusieurs séances de pratique et ceux qui n'en ont reçu aucun.
Figures
Comment in
-
This resident has got to learn!Can J Surg. 2005 Jun;48(3):181-3. Can J Surg. 2005. PMID: 16013620 Free PMC article. No abstract available.
-
Surgical training.Can J Surg. 2005 Oct;48(5):419; author reply 419. Can J Surg. 2005. PMID: 16248147 Free PMC article. No abstract available.
Similar articles
-
The effectiveness of video feedback in the acquisition of orthopedic technical skills.Am J Surg. 2004 Mar;187(3):427-32. doi: 10.1016/j.amjsurg.2003.12.011. Am J Surg. 2004. PMID: 15006577 Clinical Trial.
-
Standardization is superior to traditional methods of teaching open vascular simulation.J Vasc Surg. 2011 Jan;53(1):229-234, 235.e1-2; discussion 234-5. doi: 10.1016/j.jvs.2010.07.064. Epub 2010 Nov 5. J Vasc Surg. 2011. PMID: 21115317 Clinical Trial.
-
Evaluation of simulation-based training model on vascular anastomotic skills for surgical residents.Simul Healthc. 2012 Dec;7(6):334-8. doi: 10.1097/SIH.0b013e318264655e. Simul Healthc. 2012. PMID: 22960701
-
Core training in surgery: what does it need to include?Semin Vasc Surg. 2006 Dec;19(4):210-3. doi: 10.1053/j.semvascsurg.2006.08.010. Semin Vasc Surg. 2006. PMID: 17178325 Review.
-
Intraoperative Teaching and Evaluation in General Surgery.Surg Clin North Am. 2021 Aug;101(4):587-595. doi: 10.1016/j.suc.2021.05.006. Surg Clin North Am. 2021. PMID: 34242602 Review.
Cited by
-
Effect of face-to-face verbal feedback compared with no or alternative feedback on the objective workplace task performance of health professionals: a systematic review and meta-analysis.BMJ Open. 2020 Mar 25;10(3):e030672. doi: 10.1136/bmjopen-2019-030672. BMJ Open. 2020. PMID: 32213515 Free PMC article.
-
Can both residents and chief physicians assess surgical skills?Surg Endosc. 2012 Jul;26(7):2054-60. doi: 10.1007/s00464-012-2155-1. Epub 2012 Jan 20. Surg Endosc. 2012. PMID: 22271335
-
Minimally invasive tele-mentoring opportunity-the mito project.Surg Endosc. 2020 Jun;34(6):2585-2592. doi: 10.1007/s00464-019-07024-1. Epub 2019 Jul 30. Surg Endosc. 2020. PMID: 31363891
-
Video Modeling and Video Feedback to Reduce Time to Perform Intravenous Cannulation in Medical Students: A Randomized-Controlled Mixed-Methods Study.Can J Anaesth. 2020 Jun;67(6):715-725. doi: 10.1007/s12630-020-01570-2. Epub 2020 Jan 22. Can J Anaesth. 2020. PMID: 32052372 Clinical Trial. English.
-
Video-based coaching in surgical education: a systematic review and meta-analysis.Surg Endosc. 2020 Feb;34(2):521-535. doi: 10.1007/s00464-019-07265-0. Epub 2019 Nov 20. Surg Endosc. 2020. PMID: 31748927
References
-
- Barnes RW. Surgical handicraft: teaching and learning surgical skills. Am J Surg 1987;153:422-7. - PubMed
-
- Winckel P, Reznick R, Cohen R, Taylor B. Reliability and construct validity of a structured technical skills assessment form. Am J Surg 1994;167:423-7. - PubMed
-
- Heppell J, Beauchamp G, Chollet A. Ten-year experience with a basic technical skills and perioperative management workshop for first-year residents. Can J Surg 1995;38:27-32. - PubMed
-
- Martin JA, Regehr G, Reznick R, MacRae H, Murnaghan J, Hutchison C, et al. Objective structured assessment of technical skill (OSATS) for surgical residents. Br J Surg 1997;84:273-8. - PubMed
-
- Reznick R, Regehr G, MacRae H, Martin J, McCulloch W. Testing technical skill via an innovative “bench station” examination. Am J Surg 1997;173:226-30. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical