

Treatment and outcome of vertebral Langerhans cell histiocytosis at the Children's Hospital of Eastern Ontario
- PMID: 16013628
- PMCID: PMC3211544
Treatment and outcome of vertebral Langerhans cell histiocytosis at the Children's Hospital of Eastern Ontario
Abstract
Background: We wished to evaluate the treatment methods for vertebral Langerhans cell histiocytosis (LCH) (a rare reticuloendothelial disorder) at a tertiary care pediatric centre and compare treatment and outcomes with those reported in the recent literature.
Methods: A total of 55 charts were retrieved between 1980 and 2003 for children with LCH. Only those children who were under 18 years of age, had a diagnosis of LCH, histiocytosis X or eosinophilic granuloma and had documented vertebral involvement were included. The data collected were compared with data in the literature with respect to epidemiologic features, symptoms, investigations and procedures done, treatment, outcome and follow-up.
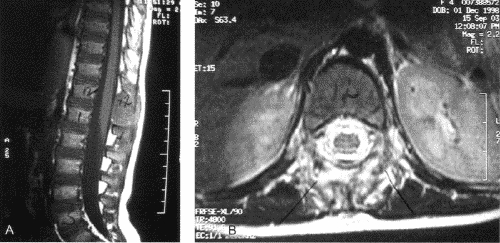
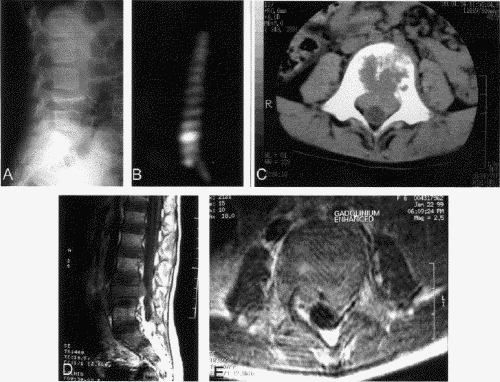
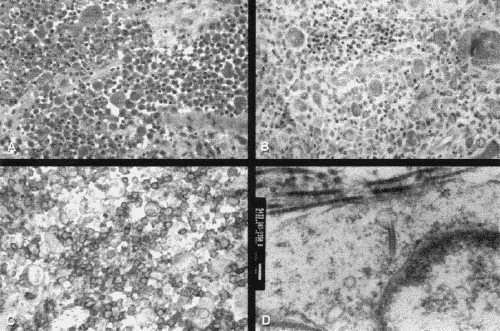
Results: Of the 8 children who met the inclusion criteria for vertebral LCH, the most common presenting complaint was back or neck pain. The thoracic vertebrae were most commonly affected followed equally by cervical and lumbar spines. Most children underwent a complete diagnostic work-up. A single solitary lesion was found in only 1 child. Biopsies were attempted in all cases with 6 positive results. Treatment varied depending on the severity of the presenting complaint; however, none of the tumours was completely resected. Follow-up averaged 3.4 years, and only 1 child has had a recurrence.
Conclusion: A multidisciplinary investigation is recommended for children with suspected vertebral LCH. Treatment depends on the severity of the disease.
Contexte: Nous voulions évaluer les méthodes de traitement de l'histiocytose vertébrale à cellules de Langerhans (HCL) (trouble rare du système réticuloendothélial) à un centre pédiatrique de soins tertiaires et comparer le traitement et les résultats à ceux que l'on signale dans des publications récentes.
Méthodes: On a extrait au total 55 dossiers d'enfants atteints d'HCL entre 1980 et 2003. On a inclus seulement les enfants de moins de 18 ans, chez lesquels on avait diagnostiqué une HCL, une histiocytose X ou un granulome à éosinophiles et une atteinte vertébrale documentée. On a comparé les données recueillies à celles des publications sur les plans des caractéristiques épidémiologique, des symptômes, des investigations et des interventions pratiquées, des traitements, des résultats et des suivis.
Résultats: Les huit enfants qui satisfaisaient aux critères d'inclusion se plaignaient le plus souvent de douleur au dos ou au cou. Les vertèbres thoraciques étaient les plus souvent atteintes, suivies également par les cervicales et les lombaires. La plupart des enfants ont subi des examens complets de diagnostic. On a trouvé une seule lésion isolée chez un enfant seulement. On a pratiqué une biopsie dans tous les cas et obtenu six résultats positifs. Le traitement a varié selon la gravité de la plainte, mais aucune des tumeurs n'a été réséquée complètement. Le suivi a duré en moyenne 3,4 ans et il y a eu récidive chez un enfant seulement.
Conclusion: On recommande une investigation multidisciplinaire dans le cas des enfants chez lesquels on soupçonne une HCL vertébrale. Le traitement dépend de la gravité de la maladie.
Figures
References
-
- Bertram C, Madert J, Eggers C. Eosinophilic granuloma of the cervical spine [review]. Spine 2002;27:1408-13. - PubMed
-
- Hanapiah F, Yaacob H, Ghani KS, Hussin AS. Histiocytosis X: evidence for a genetic etiology. J Nihon Univ Sch Dent 1993;35: 171-4. - PubMed
-
- Favara BE, Feller AC, Pauli M, Jaffe ES, Weiss LM, Arico M, et al. Contemporary classification of histiocytic disorders. The WHO Committee On Histiocytic/Reticulum Cell Proliferations. Reclassification Working Group of the Histiocyte Society [review]. Med Pediatr Oncol 1997;29:157-66. - PubMed
-
- Dickinson LD, Farhat SM. Eosinophilic granuloma of the cervical spine. A case report and review of the literature. Surg Neurol 1991;35:57-63. - PubMed
-
- Gandolfi A. Vertebral histiocytosis-X causing spinal cord compression. Surg Neurol 1983;19:369-72. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous