

Effect of prone positioning on clinical outcomes in children with acute lung injury: a randomized controlled trial
- PMID: 16014597
- PMCID: PMC1237036
- DOI: 10.1001/jama.294.2.229
Effect of prone positioning on clinical outcomes in children with acute lung injury: a randomized controlled trial
Abstract
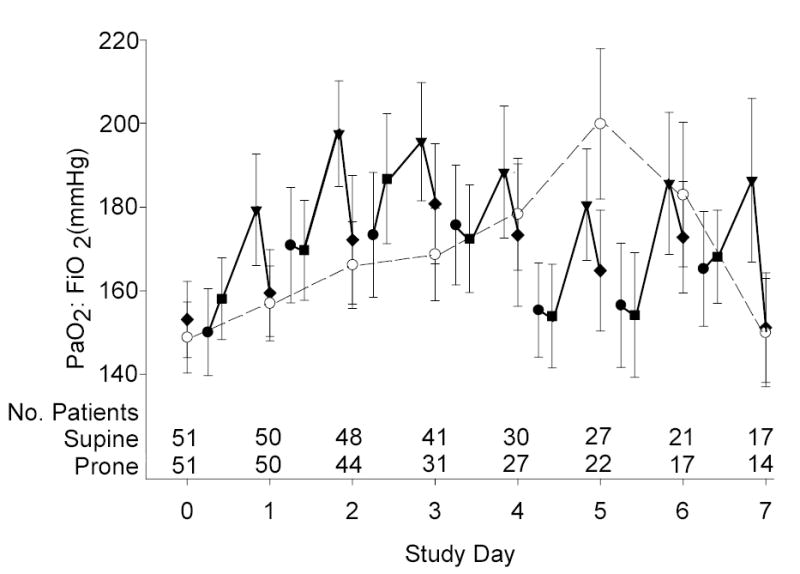
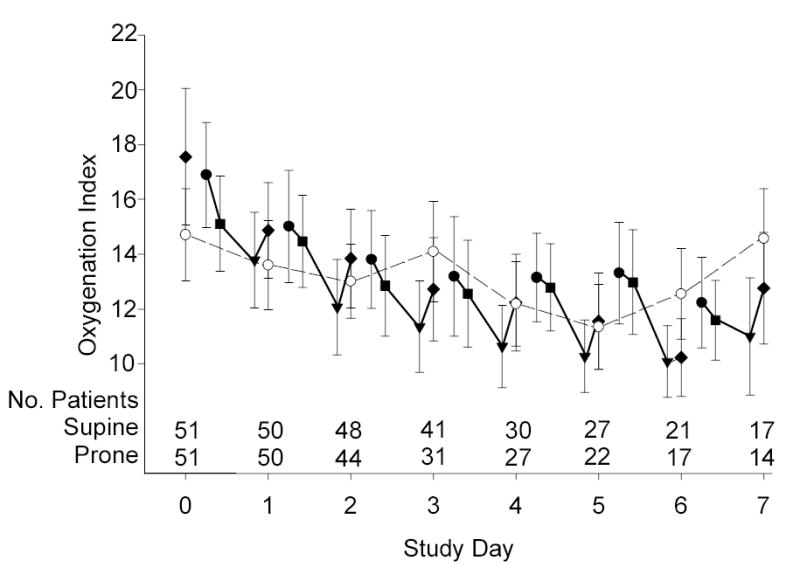
Context: In uncontrolled clinical studies, prone positioning appeared to be safe and to improve oxygenation in pediatric patients with acute lung injury. However, the effect of prone positioning on clinical outcomes in children is not known.
Objective: To test the hypothesis that at the end of 28 days infants and children with acute lung injury treated with prone positioning would have more ventilator-free days than those treated with supine positioning.
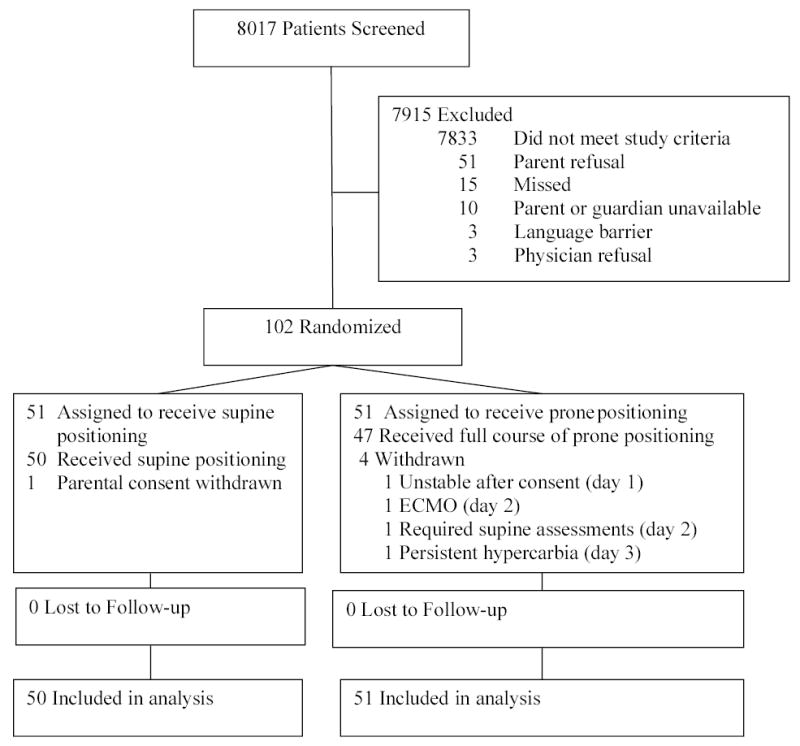
Design, setting, and patients: Multicenter, randomized, controlled clinical trial conducted from August 28, 2001, to April 23, 2004, of 102 pediatric patients from 7 US pediatric intensive care units aged 2 weeks to 18 years who were treated with supine vs prone positioning. Randomization was concealed and group assignment was not blinded.
Intervention: Patients were randomized to either supine or prone positioning within 48 hours of meeting acute lung injury criteria, with those patients in the prone group being positioned within 4 hours of randomization and remaining prone for 20 hours each day during the acute phase of their illness for a maximum of 7 days, after which they were positioned supine. Both groups were treated using lung protective ventilator and sedation protocols, extubation readiness testing, and hemodynamic, nutrition, and skin care guidelines.
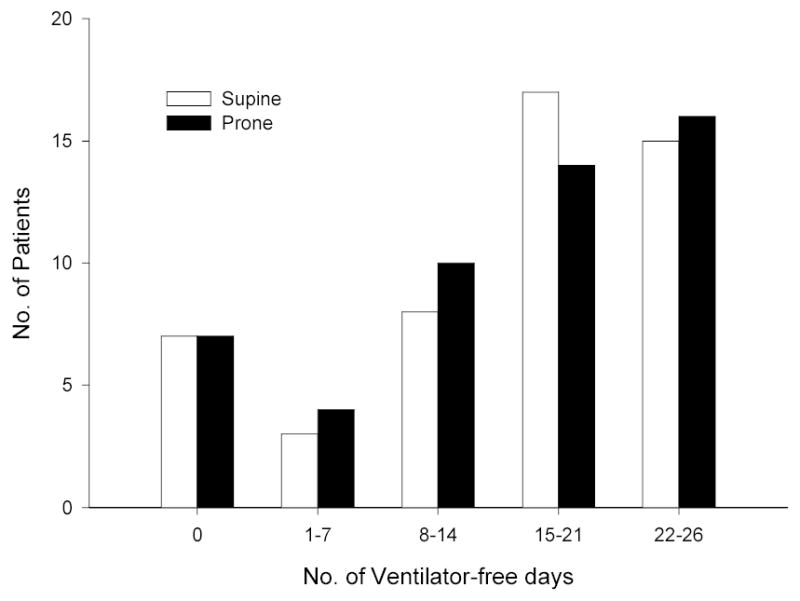
Main outcome measure: Ventilator-free days to day 28.
Results: The trial was stopped at the planned interim analysis on the basis of the prespecified futility stopping rule. There were no differences in the number of ventilator-free days between the 2 groups (mean [SD], 15.8 [8.5] supine vs 15.6 [8.6] prone; mean difference, -0.2 days; 95% CI, -3.6 to 3.2; P = .91). After controlling for age, Pediatric Risk of Mortality III score, direct vs indirect acute lung injury, and mode of mechanical ventilation at enrollment, the adjusted difference in ventilator-free days was 0.3 days (95% CI, -3.0 to 3.5; P = .87). There were no differences in the secondary end points, including proportion alive and ventilator-free on day 28 (P = .45), mortality from all causes (P>.99), the time to recovery of lung injury (P = .78), organ-failure-free days (P = .88), and cognitive impairment (P = .16) or overall functional health (P = .12) at hospital discharge or on day 28.
Conclusion: Prone positioning does not significantly reduce ventilator-free days or improve other clinical outcomes in pediatric patients with acute lung injury.
Figures
Comment in
-
Prone positioning in children with ARDS: positive reflections on a negative clinical trial.JAMA. 2005 Jul 13;294(2):248-50. doi: 10.1001/jama.294.2.248. JAMA. 2005. PMID: 16014601 No abstract available.
-
Prone positioning in children with acute lung injury.JAMA. 2005 Nov 9;294(18):2297; author reply 2297-8. doi: 10.1001/jama.294.18.2297-a. JAMA. 2005. PMID: 16278352 No abstract available.
References
-
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1334–1349. - PubMed
-
- ARDS Clinical Trials Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301–1308. - PubMed
-
- Dreyfuss D, Soler P, Basset G, Saumon G. High inflation pressure pulmonary edema. Respective effects of high airway pressure, high tidal volume, and positive end-expiratory pressure. Am Rev Respir Dis. 1988;137(5):1159–1164. - PubMed
-
- Muscedere JG, Mullen JB, Gan K, Slutsky AS. Tidal ventilation at low airway pressures can augment lung injury. Am J Respir Crit Care Med. 1994;149(5):1327–1334. - PubMed
-
- Bryan AC. Comments of a devil’s advocate. Am Rev Respir Dis. 1974;110:143–144. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
