

Gastrin and antral G cells in course of Helicobacter pylori eradication: six months follow up study
- PMID: 16015680
- PMCID: PMC4615433
- DOI: 10.3748/wjg.v11.i27.4140
Gastrin and antral G cells in course of Helicobacter pylori eradication: six months follow up study
Abstract
Aim: To assess long-term effects of Helicobacter pylori (H pylori) eradication on antral G cell morphology and function in patients with and without duodenal ulcer (DU).
Methods: Consecutive dyspeptic patients referred to the endoscopy entered the study. Out of 39 H pylori positive patients, 8 had DU (H pylori +DU) and 31 gastritis (H pylori +G). Control groups consisted of 11 uninfected dyspeptic patients (CG1) and 7 healthy volunteers (CG2). Basal plasma gastrin (PGL), antral tissue gastrin concentrations (ATGC), immunohistochemical and electron microscopic characteristics of G cells were determined, prior to and 6 mo after therapy.
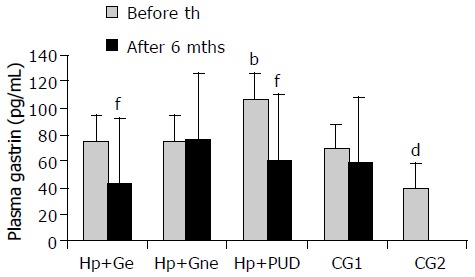
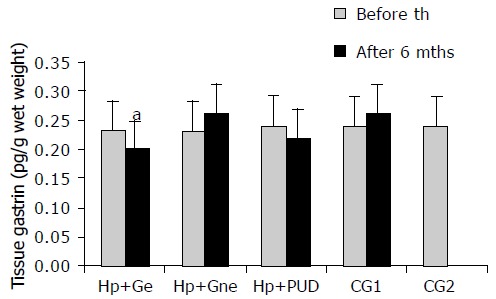
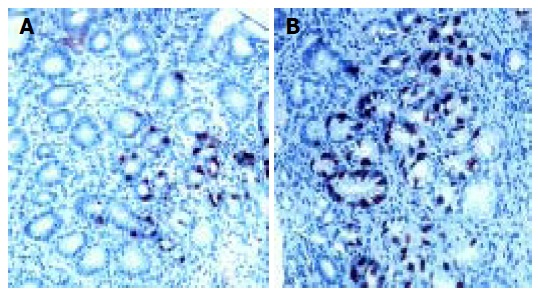
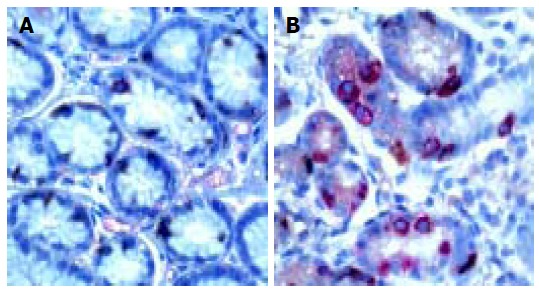
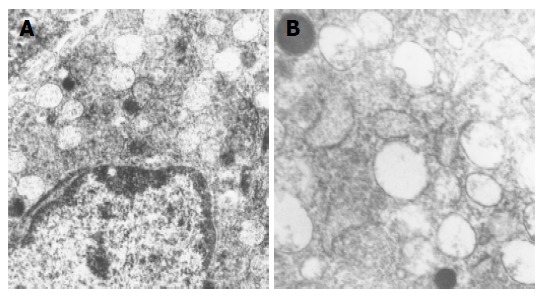
Results: We demonstrated elevated PGL in infected patients compared to uninfected controls prior to therapy. Elevated PGL were registered in all H pylori+patients (H pylori +DU: 106.78+/-22.72 pg/mL, H pylori +G: 74.95+/-15.63, CG1: 68.59+/-17.97, CG2: 39.24+/-5.59 pg/mL, P<0.01). Successful eradication (e) therapy in H pylori+patients lead to significant decrease in PGL (H pylori+DU: 59.93+/-9.40 and H pylori +Ge: 42.36+/-10.28 pg/mL, P<0.001). ATGC at the beginning of the study were similar in infected and uninfected patients and eradication therapy lead to significant decrease in ATGC in H pylori +gastritis, but not in DU patients. In the H pylori +DU patients, the mean number of antral G cells was significantly lower in comparison with all other groups (P<0.01), but after successful eradication was close to normal values found in controls. By contrast, G cell number and volume density were significantly decreased (P<0.01) in H pylori +Ge group after successful eradication therapy (294+/-32 and 0.31+/-0.02, respectively), in comparison to values before eradication (416+/-40 and 0.48+/-0.09). No significant change of the G cell/total endocrine cell ratio was observed during the 6 mo of follow up in any of the groups. A reversible increase in G cell secretory function was seen in all infected individuals, demonstrated by a more prominent secretory apparatus. However, differences between DU and gastritis group were identified.
Conclusion: H pylori infection induces antral G cell hyperfunction resulting in increased gastrin synthesis and secretion. After eradication therapy complete morphological and functional recovery is observed in patients with gastritis. In the DU patients some other factors unrelated to the H pylori infection influence antral G cell morphology and function.
Figures

References
-
- Bobrzyński A. Hormonal, secretory and morphological alterations in gastric mucosa in the course of Helicobacter pylori eradication in patients with duodenal ulcer and non-ulcer dyspepsia. J Physiol Pharmacol. 1997;48 Suppl 3:1–56. - PubMed
-
- Hunt RH, Huang JQ. The case for treatment of dyspeptic patients infected with H. pylori. Eur J Surg Suppl. 1998;582:6–10. - PubMed
-
- Kaneko H, Konagaya T, Kusugami K. Helicobacter pylori and gut hormones. J Gastroenterol. 2002;37:77–86. - PubMed
-
- Gisbert JP, Boixeda D, Vila T, de Rafael L, Redondo C, de Argila CM. Basal and stimulated gastrin levels and gastric acid output five months after therapy for Helicobacter pylori eradication in duodenal ulcer patients. J Clin Gastroenterol. 1996;22:90–95. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
