

The physiological challenges of the 1952 Copenhagen poliomyelitis epidemic and a renaissance in clinical respiratory physiology
- PMID: 16020437
- PMCID: PMC1351016
- DOI: 10.1152/japplphysiol.00184.2005
The physiological challenges of the 1952 Copenhagen poliomyelitis epidemic and a renaissance in clinical respiratory physiology
Abstract
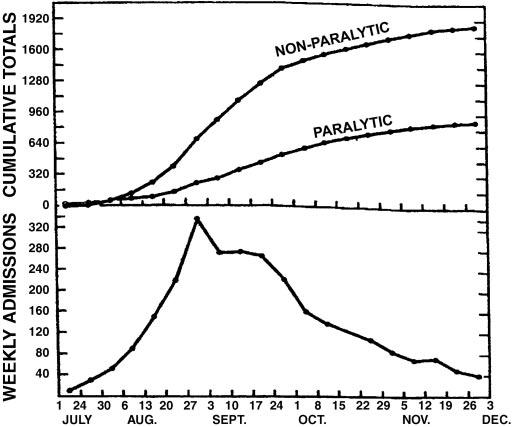
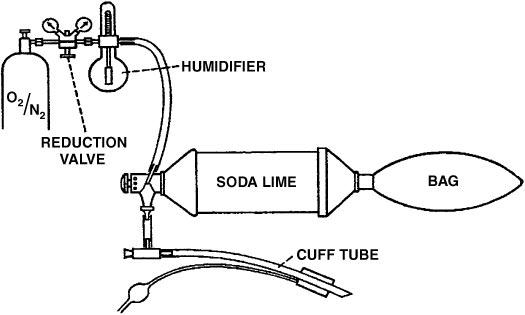
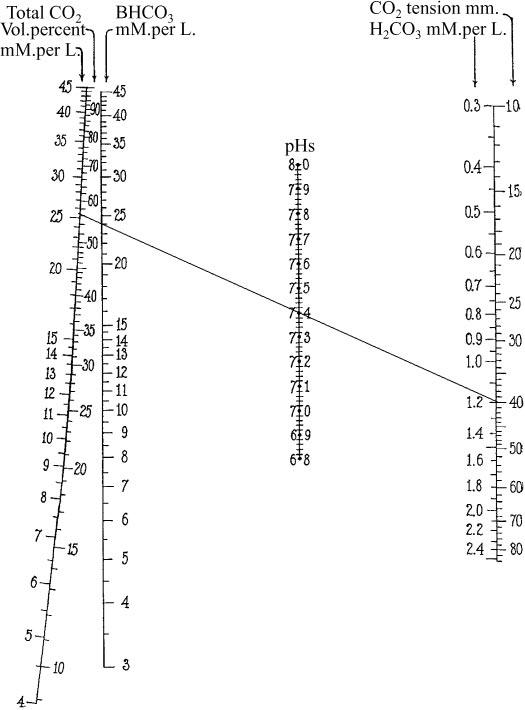
The 1952 Copenhagen poliomyelitis epidemic provided extraordinary challenges in applied physiology. Over 300 patients developed respiratory paralysis within a few weeks, and the ventilator facilities at the infectious disease hospital were completely overwhelmed. The heroic solution was to call upon 200 medical students to provide round-the-clock manual ventilation using a rubber bag attached to a tracheostomy tube. Some patients were ventilated in this way for several weeks. A second challenge was to understand the gas exchange and acid-base status of these patients. At the onset of the epidemic, the only measurement routinely available in the hospital was the carbon dioxide concentration in the blood, and the high values were initially misinterpreted as a mysterious "alkalosis." However, pH measurements were quickly instituted, the Pco(2) was shown to be high, and modern clinical respiratory acid-base physiology was born. Taking a broader view, the problems highlighted by the epidemic underscored the gap between recent advances made by physiologists and their application to the clinical environment. However, the 1950s ushered in a renaissance in clinical respiratory physiology. In 1950 the coverage of respiratory physiology in textbooks was often woefully inadequate, but the decade saw major advances in topics such as mechanics and gas exchange. An important development was the translation of the new knowledge from departments of physiology to the clinical setting. In many respects, this period was therefore the beginning of modern clinical respiratory physiology.
Figures



References
-
- Astrup P. A simple electrometric technique for the determination of carbon dioxide tension in blood and plasma, total content of carbon dioxide in plasma, and bicarbonate content in separated plasma at a fixed carbon dioxide tension (40 mmHg) Scand J Clin Lab Invest. 1956;8:33–43. - PubMed
-
- Astrup P, Severinghaus J. The History of Blood Gases, Acids and Bases. Munksgaard; Copenhagen: 1986.
-
- Best CH, Taylor NB. The Physiological Basis of Medical Practice. Williams & Wilkins; Baltimore, MD: 1950.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous