

Myocardial late gadolinium enhancement cardiovascular magnetic resonance in hypertrophic cardiomyopathy caused by mutations in troponin I
- PMID: 16020591
- PMCID: PMC1769031
- DOI: 10.1136/hrt.2004.041384
Myocardial late gadolinium enhancement cardiovascular magnetic resonance in hypertrophic cardiomyopathy caused by mutations in troponin I
Abstract
Objective: To examine the influence of genotype on late gadolinium enhancement (LGE) and the potential of cardiovascular magnetic resonance (CMR) to detect preclinical hypertrophic cardiomyopathy.
Design: Prospective, blinded cohort study of myocardial LGE in a genetically homogeneous population.
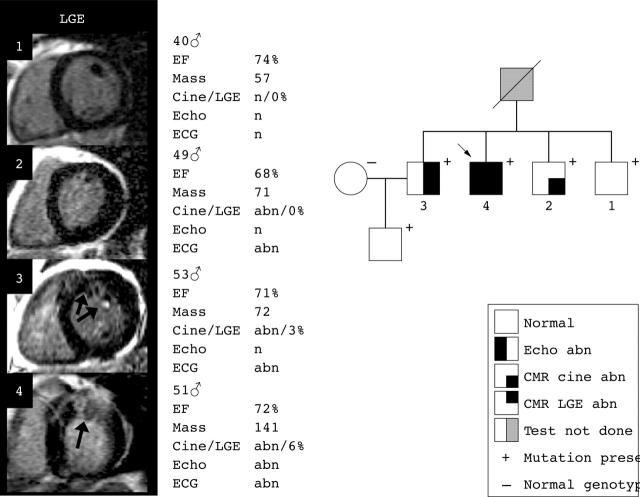
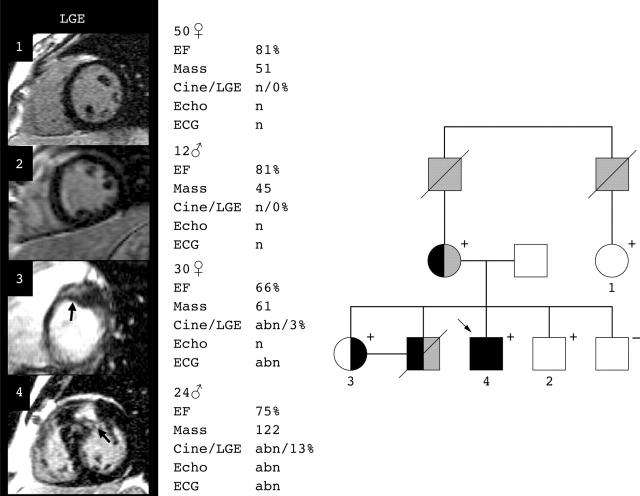
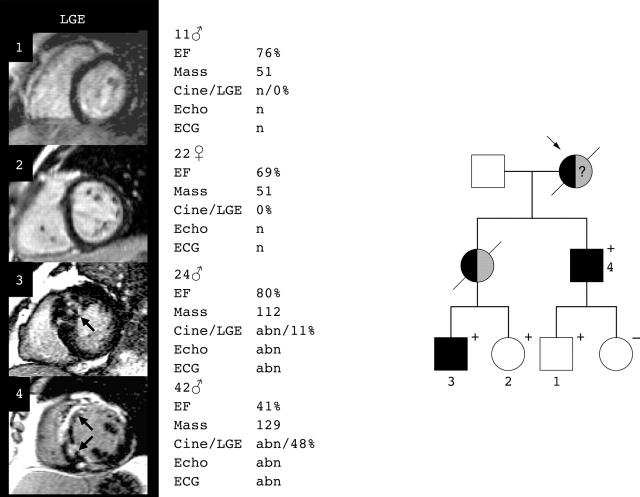
Patients: 30 patients with disease causing mutations in the recognised hypertrophic cardiomyopathy gene for cardiac troponin I (TNNI3): 15 with echocardiographically determined left ventricular hypertrophy (LVH+) and 15 without (LVH-).
Main outcome measures: CMR measures of regional left ventricular function, wall thickness, and mass, and the extent and distribution of LGE.
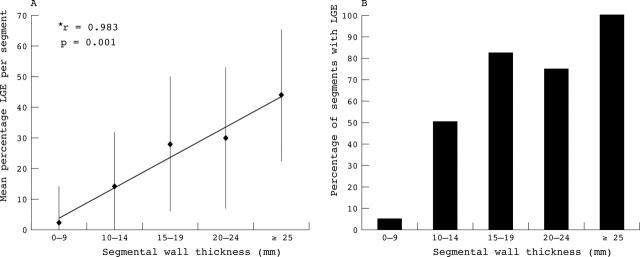
Results: LGE was found in 12 (80%) LVH+ patients but with variable extent (mean 15%, range 3-48%). LGE was also found in two (13%) LVH- patients but the extent was limited (3.6%) and both patients were found to have an abnormal ECG and regional hypertrophy by cine CMR. The extent of LGE was positively associated with clinical markers of sudden death risk (21% with > or = 2 risk factors v 7% with < or = 1 risk factor, p = 0.02) and left ventricular mass (r = 0.56, p < 0.001) and was inversely associated with ejection fraction (r = -0.58, p < 0.001). Segmental analysis showed that as regional wall thickness increased, LGE was more prevalent (p < 0.0001) and more extensive (r = 0.98, p = 0.001).
Conclusion: In patients with disease causing mutations in TNNI3, focal fibrosis was not detected by LGE CMR before LVH and ECG abnormalities were present. Once LVH is present, LGE is common and the extent correlates with adverse clinical parameters. This suggests that focal fibrosis is closely linked to disease development.
Figures
References
-
- Maron BJ, McKenna WJ, Danielson, et al. American College of Cardiology/European Society of Cardiology clinical expert consensus document on hypertrophic cardiomyopathy. J Am Coll Cardiol 2003;42:1687–713. - PubMed
-
- Richardson P, McKenna W, Bristow M, et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology task force on the definition and classification of cardiomyopathies. Circulation 1996;93:841–2. - PubMed
-
- Anderson KR, Sutton MG, Lie JT. Histopathological types of cardiac fibrosis in myocardial disease. J Pathol 1979;128:79–85. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials