

Timing of presentation and postnatal outcome of infants suspected of having coarctation of the aorta during fetal life
- PMID: 16020599
- PMCID: PMC1769023
- DOI: 10.1136/hrt.2003.033027
Timing of presentation and postnatal outcome of infants suspected of having coarctation of the aorta during fetal life
Abstract
Objective: To report the timing of presentation and clinical profile of a cohort of fetuses with normal main cardiac connections but fetal echocardiographic signs suggestive of coarctation of the aorta.
Design: Retrospective observational study.
Setting: Tertiary fetal and paediatric cardiology centre.
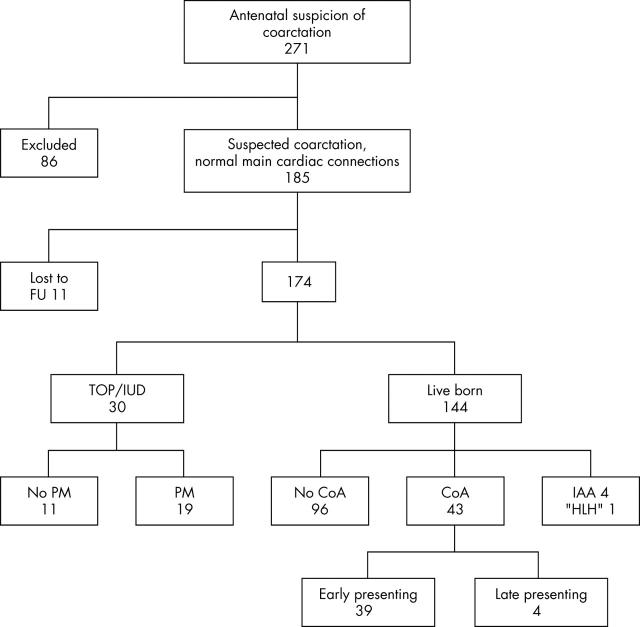
Patients: Between 1 January 1998 and 31 December 2002, 174 fetuses were studied, of whom 144 infants were born alive.
Main outcome measures: Of the 144 liveborn infants, 43 had coarctation of the aorta, four had interruption of the aortic arch, and one was managed as having hypoplastic left heart syndrome. Hemianomalous pulmonary venous drainage was diagnosed in two infants. Three infants with coarctation presented late at 7-13 weeks of age, 6-12 weeks after closure of the arterial duct. Fetuses with cardiac asymmetry had a higher incidence of left superior vena cava than a control group. For fetuses with cardiac asymmetry, the incidence of left superior vena cava and ventricular septal defects was similar in infants who proved to have coarctation postnatally and in those who did not. The 30 day and one year surgical mortality of infants having repair of coarctation of the aorta was two of 41 (4.9%, 95% confidence interval (CI) 0.6 to 16.0). All cause mortality of liveborn infants with any abnormality of the aortic arch was five of 48 (10.4%, 95% CI 3.5 to 22.7) at 30 days and one year, which was heavily influenced by prematurity and extracardiac abnormalities.
Conclusions: Precise diagnosis of coarctation of the aorta during fetal life remains difficult. Coarctation of the aorta may present several weeks after closure of the arterial duct and sequential echocardiography is recommended.
Figures
References
-
- Allan LD, Sharland GK, Milburn A, et al. Prospective diagnosis of 1006 consecutive cases of congenital heart disease in the fetus. J Am Coll Cardiol 1994;23:1452–8. - PubMed
-
- Hornberger LK, Sahn DJ, Kleinman CS, et al. Antenatal diagnosis of coarctation of the aorta: a multicentre experience. J Am Coll Cardiol 1994;23:417–23. - PubMed
-
- Hornberger LK. Aortic arch anomalies. In: Lindsey A, Lisa H, Gurleen S, eds. Textbook of fetal cardiology. London: Greenwich Medical Media, 2000:307–31.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical