

Novel perspectives on mucormycosis: pathophysiology, presentation, and management
- PMID: 16020690
- PMCID: PMC1195964
- DOI: 10.1128/CMR.18.3.556-569.2005
Novel perspectives on mucormycosis: pathophysiology, presentation, and management
Abstract
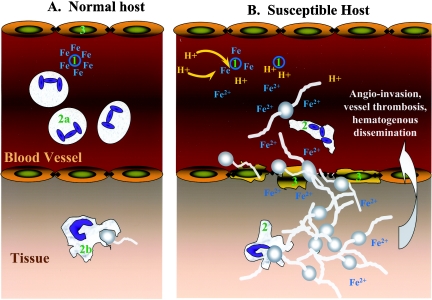
Mucormycosis is a life-threatening fungal infection that occurs in immunocompromised patients. These infections are becoming increasingly common, yet survival remains very poor. A greater understanding of the pathogenesis of the disease may lead to future therapies. For example, it is now clear that iron metabolism plays a central role in regulating mucormycosis infections and that deferoxamine predisposes patients to mucormycosis by inappropriately supplying the fungus with iron. These findings raise the possibility that iron chelator therapy may be useful to treat the infection as long as the chelator does not inappropriately supply the fungus with iron. Recent data support the concept that high-dose liposomal amphotericin is the preferred monotherapy for mucormycosis. However, several novel therapeutic strategies are available. These options include combination therapy using lipid-based amphotericin with an echinocandin or with an azole (largely itraconazole or posaconazole) or with all three. The underlying principles of therapy for this disease remain rapid diagnosis, reversal of underlying predisposition, and urgent surgical debridement.
Figures
References
-
- Abe, F., H. Inaba, T. Katoh, and M. Hotchi. 1990. Effects of iron and desferrioxamine on Rhizopus infection. Mycopathologia 110:87-91. - PubMed
-
- Abedi, E., A. Sismanis, K. Choi, and P. Pastore. 1984. Twenty-five years' experience treating cerebro-rhino-orbital mucormycosis. Laryngoscope 94:1060-1062. - PubMed
-
- Abzug, M. J., and T. J. Walsh. 2004. Interferon-gamma and colony-stimulating factors as adjuvant therapy for refractory fungal infections in children. Pediatr. Infect. Dis. J. 23:769-773. - PubMed
-
- Adam, R. D., G. Hunter, J. DiTomasso, and G. Comerci, Jr. 1994. Mucormycosis: emerging prominence of cutaneous infections. Clin. Infect. Dis. 19:67-76. - PubMed
-
- Alsuwaida, K. 2002. Primary cutaneous mucormycosis complicating the use of adhesive tape to secure the endotracheal tube. Can. J. Anaesth. 49:880-882. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
