

Plasmodium ovale: parasite and disease
- PMID: 16020691
- PMCID: PMC1195966
- DOI: 10.1128/CMR.18.3.570-581.2005
Plasmodium ovale: parasite and disease
Abstract
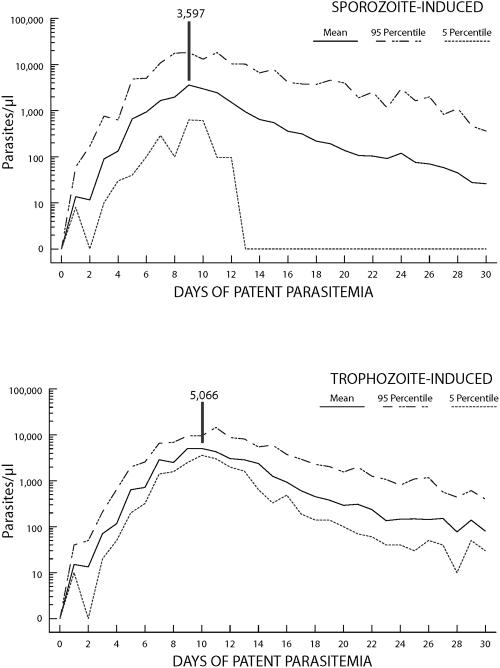
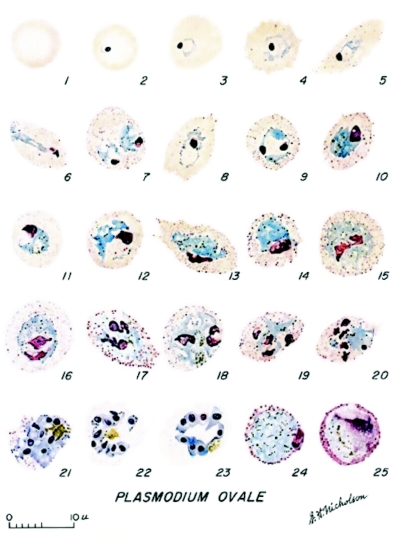
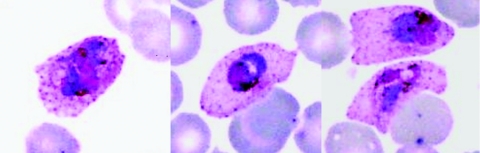
Humans are infected by four recognized species of malaria parasites. The last of these to be recognized and described is Plasmodium ovale. Like the other malaria parasites of primates, this parasite is only transmitted via the bites of infected Anopheles mosquitoes. The prepatent period in the human ranges from 12 to 20 days. Some forms in the liver have delayed development, and relapse may occur after periods of up to 4 years after infection. The developmental cycle in the blood lasts approximately 49 h. An examination of records from induced infections indicated that there were an average of 10.3 fever episodes of > or = 101 degrees F and 4.5 fever episodes of > or = 104 degrees F. Mean maximum parasite levels were 6,944/microl for sporozoite-induced infections and 7,310/microl for trophozoite-induced infections. Exoerythrocytic stages have been demonstrated in the liver of humans, chimpanzees, and Saimiri monkeys following injection of sporozoites. Many different Anopheles species have been shown to be susceptible to infection with P. ovale, including A. gambiae, A. atroparvus, A. dirus, A. freeborni, A. albimanus, A. quadrimaculatus, A. stephensi, A. maculatus, A. subpictus, and A. farauti. An enzyme-linked immunosorbent assay has been developed to detect mosquitoes infected with P. ovale using a monoclonal antibody directed against the circumsporozoite protein. Plasmodium ovale is primarily distributed throughout sub-Saharan Africa. It has also been reported from numerous islands in the western Pacific. In more recent years, there have been reports of its distribution on the Asian mainland. Whether or not it will become a major public health problem there remains to be seen. The diagnosis of P. ovale is based primarily on the characteristics of the blood stages and its differentiation from P. vivax. The sometimes elliptical shape of the infected erythrocyte is often diagnostic when combined with other, subtler differences in morphology. The advent of molecular techniques, primarily PCR, has made diagnostic confirmation possible. The development of techniques for the long-term frozen preservation of malaria parasites has allowed the development diagnostic reference standards for P. ovale. Infections in chimpanzees are used to provide reference and diagnostic material for serologic and molecular studies because this parasite has not been shown to develop in other nonhuman primates, nor has it adapted to in vitro culture. There is no evidence to suggest that P. ovale is closely related phylogenetically to any other of the primate malaria parasites that have been examined.
Figures
References
-
- Afari, E. A., T. Nakano, F. Binka, S. Owusu-Agyei, and J. Asigbee. 1993. Seasonal characteristics of malaria infection in under-five children in a rural community in southern Ghana. W. Afr. J. Med. 12:39-42. - PubMed
-
- Aikawa, M., C. L. Hsieh, and L. H. Miller. 1977. Ultrastructural changes of the erythrocytic membrane in ovale-type malarial parasites. J. Parasitol. 63:152-154. - PubMed
-
- Anthony, R. L., M. J. Bangs, N. Hamzah, H. Basri, Purnomo, and B. Subianto. 1992. Heightened transmission of stable malaria in an isolated population in the highlands of Irian Jaya, Indonesia. Am. J. Trop. Med. Hyg. 47:346-356. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
