

Derivation and validation of a prognostic model for pulmonary embolism
- PMID: 16020800
- PMCID: PMC2718410
- DOI: 10.1164/rccm.200506-862OC
Derivation and validation of a prognostic model for pulmonary embolism
Abstract
Rationale: An objective and simple prognostic model for patients with pulmonary embolism could be helpful in guiding initial intensity of treatment.
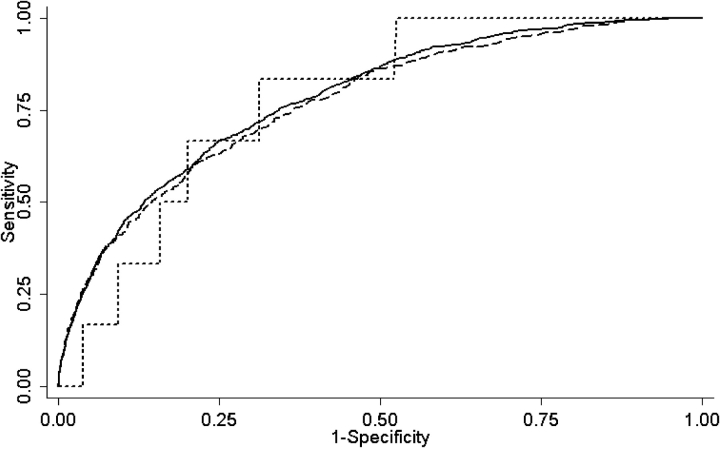
Objectives: To develop a clinical prediction rule that accurately classifies patients with pulmonary embolism into categories of increasing risk of mortality and other adverse medical outcomes.
Methods: We randomly allocated 15,531 inpatient discharges with pulmonary embolism from 186 Pennsylvania hospitals to derivation (67%) and internal validation (33%) samples. We derived our prediction rule using logistic regression with 30-day mortality as the primary outcome, and patient demographic and clinical data routinely available at presentation as potential predictor variables. We externally validated the rule in 221 inpatients with pulmonary embolism from Switzerland and France.
Measurements: We compared mortality and nonfatal adverse medical outcomes across the derivation and two validation samples.
Main results: The prediction rule is based on 11 simple patient characteristics that were independently associated with mortality and stratifies patients with pulmonary embolism into five severity classes, with 30-day mortality rates of 0-1.6% in class I, 1.7-3.5% in class II, 3.2-7.1% in class III, 4.0-11.4% in class IV, and 10.0-24.5% in class V across the derivation and validation samples. Inpatient death and nonfatal complications were <or= 1.1% among patients in class I and <or= 1.9% among patients in class II.
Conclusions: Our rule accurately classifies patients with pulmonary embolism into classes of increasing risk of mortality and other adverse medical outcomes. Further validation of the rule is important before its implementation as a decision aid to guide the initial management of patients with pulmonary embolism.
Figures
References
-
- Anderson FA Jr, Wheeler HB, Goldberg RJ, Hosmer DW, Patwardhan NA, Jovanovic B, Forcier A, Dalen JE. A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism: the Worcester DVT Study. Arch Intern Med 1991;151:933–938. - PubMed
-
- Silverstein MD, Heit JA, Mohr DN, Petterson TM, O'Fallon WM, Melton LJ III. Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med 1998;158:585–593. - PubMed
-
- Kozak LJ, Owings MF, Hall MJ. National hospital discharge survey: 2002 annual summary with detailed diagnosis and procedure data. National Center for Health Statistics. Vital Health Stat 13 2005;158:1–199. - PubMed
-
- Kurkciyan I, Meron G, Sterz F, Janata K, Domanovits H, Holzer M, Berzlanovich A, Bankl HC, Laggner AN. Pulmonary embolism as a cause of cardiac arrest: presentation and outcome. Arch Intern Med 2000;160:1529–1535. - PubMed
-
- Simonneau G, Sors H, Charbonnier B, Page Y, Laaban JP, Azarian R, Laurent M, Hirsch JL, Ferrari E, Bosson JL, et al. A comparison of low-molecular-weight heparin with unfractionated heparin for acute pulmonary embolism. The THESEE Study Group (Tinzaparine ou Heparine Standard: Evaluations dans l'Embolie Pulmonaire). N Engl J Med 1997;337:663–669. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
