

West Nile virus-associated flaccid paralysis
- PMID: 16022775
- PMCID: PMC3371783
- DOI: 10.3201/eid1107.040991
West Nile virus-associated flaccid paralysis
Abstract
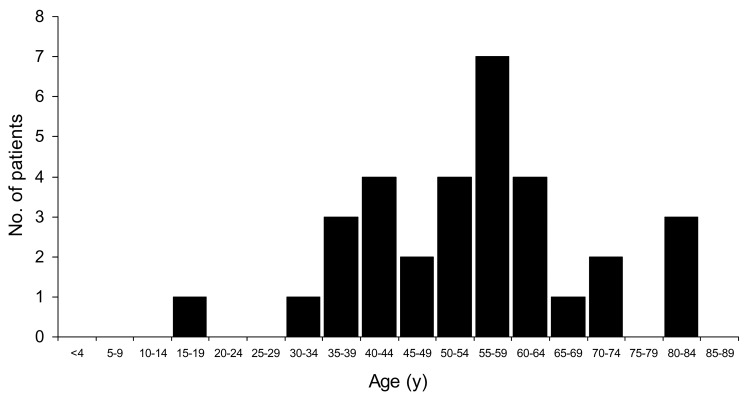
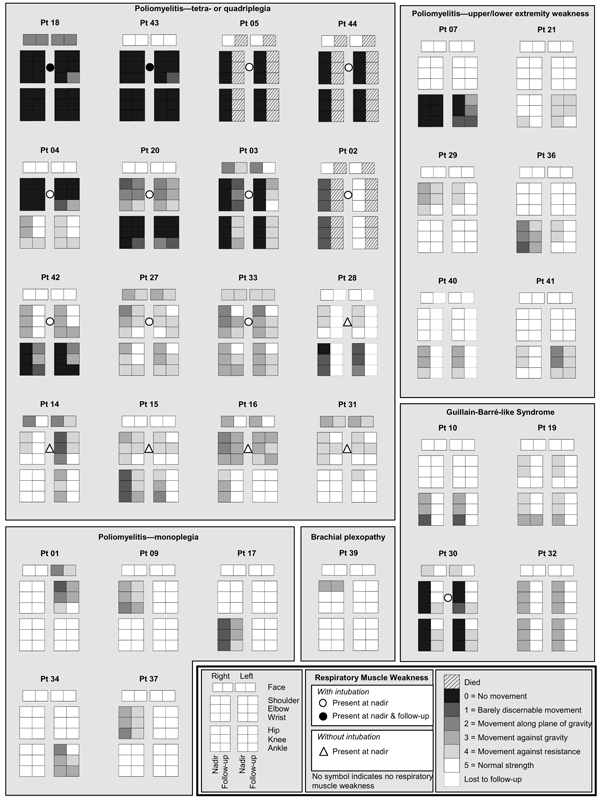
The causes and frequency of acute paralysis and respiratory failure with West Nile virus (WNV) infection are incompletely understood. During the summer and fall of 2003, we conducted a prospective, population-based study among residents of a 3-county area in Colorado, United States, with developing WNV-associated paralysis. Thirty-two patients with developing paralysis and acute WNV infection were identified. Causes included a poliomyelitislike syndrome in 27 (84%) patients and a Guillain-Barré-like syndrome in 4 (13%); 1 had brachial plexus involvement alone. The incidence of poliomyelitislike syndrome was 3.7/100,000. Twelve patients (38%), including 1 with Guillain-Barré-like syndrome, had acute respiratory failure that required endotracheal intubation. At 4 months, 3 patients with respiratory failure died, 2 remained intubated, 25 showed various degrees of improvement, and 2 were lost to followup. A poliomyelitislike syndrome likely involving spinal anterior horn cells is the most common mechanism of WNV-associated paralysis and is associated with significant short- and long-term illness and death.
Figures
Similar articles
-
West Nile virus infection presenting as acute flaccid paralysis in an HIV-infected patient: a case report and review of the literature.Neurology. 2007 Feb 13;68(7):E5-7. doi: 10.1212/01.wnl.0000253223.07720.bb. Neurology. 2007. PMID: 17296910 Review.
-
Acute flaccid paralysis: the spectrum of a newly recognized complication of West Nile virus infection.J Infect. 2005 Aug;51(2):120-7. doi: 10.1016/j.jinf.2004.10.005. Epub 2004 Nov 6. J Infect. 2005. PMID: 16038762 Review.
-
Acute flaccid paralysis syndrome associated with West Nile virus infection--Mississippi and Louisiana, July-August 2002.MMWR Morb Mortal Wkly Rep. 2002 Sep 20;51(37):825-8. MMWR Morb Mortal Wkly Rep. 2002. PMID: 12353741
-
[Flaccid paralysis associated with West Nile Virus (WNV)].Rev Invest Clin. 2004 Sep-Oct;56(5):688-90. Rev Invest Clin. 2004. PMID: 15776874 Spanish. No abstract available.
-
Posterior reversible encephalopathy syndrome resulting from Guillain-Barré-like syndrome secondary to West Nile virus infection.J Clin Neuromuscul Dis. 2011 Mar;12(3):113-7. doi: 10.1097/CND.0b013e318209ef9a. J Clin Neuromuscul Dis. 2011. PMID: 21321488
Cited by
-
PLX5622 Reduces Disease Severity in Lethal CNS Infection by Off-Target Inhibition of Peripheral Inflammatory Monocyte Production.Front Immunol. 2022 Mar 25;13:851556. doi: 10.3389/fimmu.2022.851556. eCollection 2022. Front Immunol. 2022. PMID: 35401512 Free PMC article.
-
Prolonged Zika virus viremia in a patient with Guillain-Barré syndrome in Trinidad and Tobago.Rev Panam Salud Publica. 2018 Feb 19;41:e136. doi: 10.26633/RPSP.2017.136. Rev Panam Salud Publica. 2018. PMID: 29466521 Free PMC article.
-
Ascending Trouble: Guillain-Barré-Like Syndrome Due to West Nile Virus.Cureus. 2025 Jun 2;17(6):e85240. doi: 10.7759/cureus.85240. eCollection 2025 Jun. Cureus. 2025. PMID: 40605862 Free PMC article.
-
Elsberg Syndrome with Mixed Presentation as Meningitis Retention Syndrome: A Pediatric Case Report and Comprehensive Review of the Literature.Children (Basel). 2023 Apr 14;10(4):724. doi: 10.3390/children10040724. Children (Basel). 2023. PMID: 37189973 Free PMC article.
-
Differential susceptibility of human motor neurons to infection with Usutu and West Nile virus.J Neuroinflammation. 2024 Sep 27;21(1):236. doi: 10.1186/s12974-024-03228-y. J Neuroinflammation. 2024. PMID: 39334427 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical