

Prostate cancer clinical trial end points: "RECIST"ing a step backwards
- PMID: 16033840
- PMCID: PMC1852496
- DOI: 10.1158/1078-0432.CCR-05-0109
Prostate cancer clinical trial end points: "RECIST"ing a step backwards
Abstract
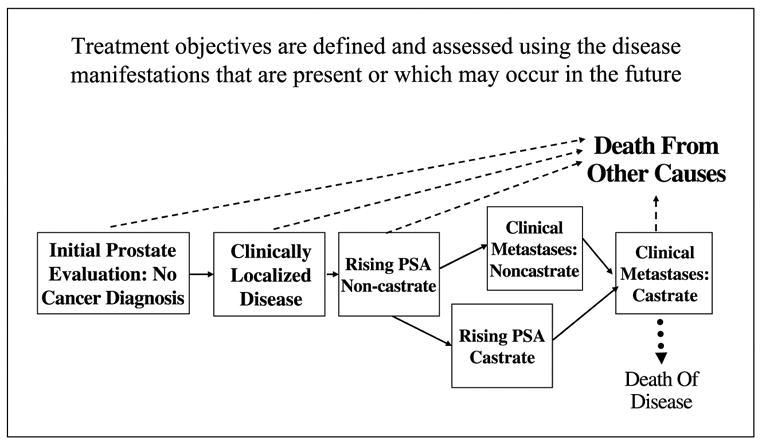
Purpose: To relate clinical issues to the clinical manifestations of prostate cancers across disease states using the eligibility and outcome criteria defined by Response Evaluation Criteria in Solid Tumors (RECIST).
Experimental design: The manifestations of prostate cancer that characterize localized, recurrent, and metastatic disease were considered using the eligibility criteria for trials defined by RECIST. To do so, we analyzed the sites, size, and distribution of lesions in patients enrolled on contemporary Institutional Review Board-approved trials for progressive castrate and noncastrate metastatic disease. Prostate-specific antigen (PSA) levels were also assessed. RECIST-defined outcome measures for tumor regression were then applied to the metastatic patient cohorts, and separately to the states of a rising PSA (noncastrate and castrate) and localized disease.
Results: Only 43.5% of men with castrate metastatic and 16% of noncastrate metastatic disease had measurable target lesions > 2 cm in size. Overall, 84.4% of the target lesions were lymph nodes, of which 67.7% were > or = 2 cm in the long axis. There are no target lesions in patients in the states of a rising PSA and localized disease, making them ineligible for trials under these criteria. PSA-based eligibility and outcomes under RECIST conflict with established reporting standards for the states of a rising PSA and castrate metastatic disease. The clinical manifestations of prostate cancer across multiple disease states are not addressed adequately using the eligibility criteria and outcomes measures defined by RECIST. Important treatment effects are not described.
Conclusions: Trial eligibility and end points based solely on tumor regression are not applicable to the majority of the clinical manifestations of prostate cancers representing all clinical states. Treatment effects can be described more precisely if eligibility criteria are adapted to the clinical question being addressed and clinical state under study, focusing on the duration of benefit defined biochemically, radiographically, and/or clinically.
Figures
References
-
- Johnson JR, Williams G, Pazdur R. End points and United States Food and Drug Administration approval of oncology drugs. J Clin Oncol. 2003;21:1404–11. - PubMed
-
- Yagoda A, Watson RC, Natale RB, et al. A critical analysis of response criteria in patients with prostatic cancer treated with cis-diamminedichloride platinum II. Cancer. 1979;44:1553–62. - PubMed
-
- Scher HI, Mazumdar M, Kelly WK. Clinical trials in relapsed prostate cancer: defining the target. J Natl Cancer Inst. 1996;88:1623–34. - PubMed
-
- Fazzari M, Heller G, Scher HI. The phase II/III transition: towards the proof of efficacy in cancer clinical trials. Control ClinTrials. 2000;21:360–8. - PubMed
-
- Scher HI, Yagoda A. Clinical trials in prostatic cancer: methodology and controversies. In: Bruce AW, Trachtenberg J, editors. Adenocarcinoma of the prostate. NewYork: Springer-Verlag; 1987. pp. 197–220.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
