

Adalimumab for treating rheumatoid arthritis
- PMID: 16034967
- PMCID: PMC12140617
- DOI: 10.1002/14651858.CD005113.pub2
Adalimumab for treating rheumatoid arthritis
Abstract
Background: Adalimumab is a fully human anti-TNFalpha monoclonal antibody. Published studies indicate that its use in patients with RA can be effective and safe.
Objectives: The aim of this review was to assess the efficacy and safety of adalimumab in the treatment of RA.
Search strategy: Electronic databases were searched up to August, 2004: MEDLINE, CINAHL, EBM Reviews (CDSR, ACP Journal Club, DARE and CENTRAL) and Health STAR. Conference proceedings were hand searched and pharmaceutical companies were contacted to obtain additional unpublished data from published trials. Adalimumab was searched as a text word as it is not currently indexed. The search was not limited by language, year of publication or type of publication.
Selection criteria: All randomised controlled trials (RCTs) or controlled clinical trials (CCTs) comparing adalimumab alone or in combination with DMARDs to placebo or other DMARDs.
Data collection and analysis: Two reviewers independently collected the data in a standardized form and assessed the methodological quality of the trial using validated criteria. Outcome measures included ACR and EULAR responses, DAS 28 and components of ACR response and radiographic data. Safety data were also included. Continuous data were reported as weighted mean difference (WMD) with 95% confidence interval (95%CI), absolute benefit (AB) and relative difference (RD). Dichotomous outcomes were reported as relative risk (RR) with 95% CI, absolute risk difference (ARD) or risk difference (RDiff) with 95%CI and number needed to treat (NNT) or to harm (NNH). When significant heterogeneity was not found, data were pooled.
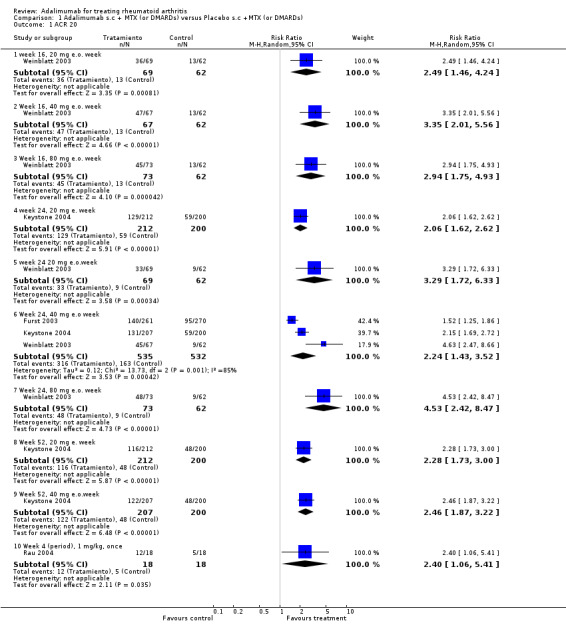
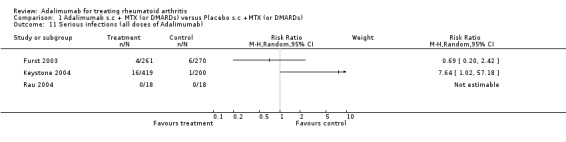
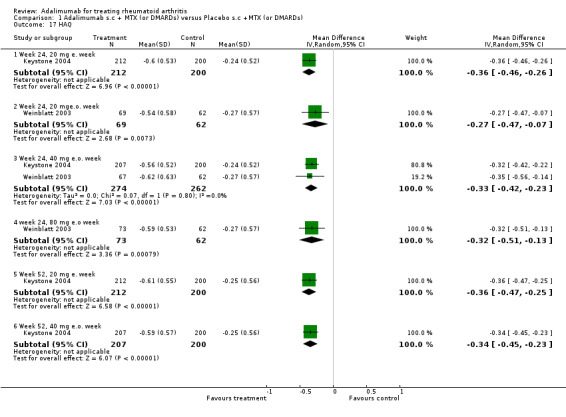
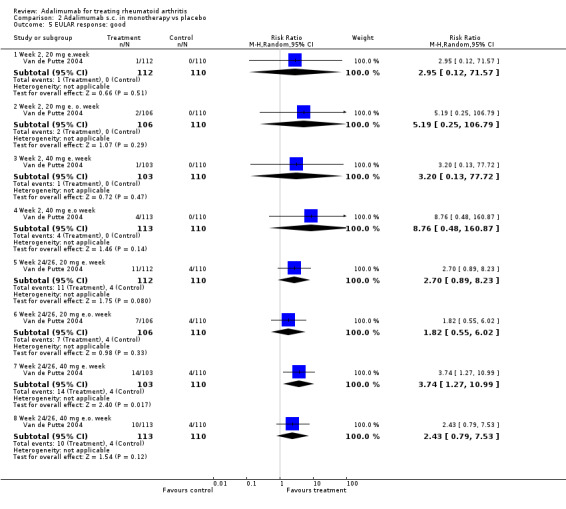
Main results: Six studies with 2381 patients were included in this review. Two comparisons were done: A. adalimumab subcutaneously (sc) + methotrexate (or DMARDs) versus placebo sc + methotrexate (or DMARDs). B. adalimumab sc in monotherapy versus placebo sc. In the comparison A, with adalimumab 40 mg every other week (e.o.w.), the RR to achieve an ACR 20 response at 24 weeks ranged in the included studies from 1.52 to 4.63, and the NNT ranged from 1.9 to 5.4. The RR (95%CI) to achieve an ACR 50 response was 4.63 (3.04-7.05), and the NNT was 3.0 (95%CI 2.0-6.0). The RR (95%CI) to achieve an ACR 70 response was 5.14 (3.14-8.41) and the number needed to treat was 7.0 (95%CI 5.0-13.0). At 52 weeks, the RRs (95%CI) to achieve an ACR 20, 50, and 70 response were 2.46 (1.87-3.22), 4.37 (2.77-6.91), and 5.15 (2.60-10.22), with NNTs of 2.9, 3.1, and 5.3, respectively. At 52 weeks, adalimumab 40 mg e.o.w. and 20 mg every week (e.w.) significantly slowed the radiological progression including Sharp modified index, erosion score, and joint space score (only with 40 mg e.o.w.). In the comparison B, with adalimumab 40 mg e.o w. , the RRs to achieve an ACR 20, 50, and 70 response at 24/26 weeks were 1.91 (1.17-3.10), 2.84 (1.58-5.12), and 7.33 (2.25-33.90) with NNTs of 5.0 (95%CI 3.0-9.0), 7.0 (4.0-20.0), and 9.0 (3.0-38.0), respectively. In most of the analysed studies and comparisons, there were not significant differences in safety outcomes between adalimumab and control groups. The development of positive antinuclear antibodies was significantly more frequent in adalimumab patients than in placebo patients. Serious infections were significantly more frequent in adalimumab patients in only one study (Keystone 2004) with a RR (95%CI) of 7.64(1.02-57.18) and a NNH of 30.2.
Authors' conclusions: On the basis of the studies reviewed here, adalimumab in combination with methotrexate is efficacious and safe in the treatment of the rheumatoid arthritis. Adalimumab 40 mg sc e.o.w. and 20 mg e.w. slows the radiographic progression at 52 weeks. Adalimumab in combination with DMARDs other than methotrexate is also efficacious and safe, even though data from one only study are available and the number of patients in each group is low. Adalimumab in monotherapy is efficacious and safe in the treatment of the rheumatoid arthritis but the effect size is lower than with combined therapy.
Conflict of interest statement
None known.
Figures









































Update of
References
References to studies included in this review
Furst 2003 {published data only}
-
- Furst DE, Schiff MH, Fleischmann RM, Strand V, Birbara CA, Compagnone D, et al. Adalimumab, a fully human anti‐tumor necrosis factor alpha monoclonal antibody, and concomitant standard antirheumatic therapy for the treatment of rheumatoid arthritis: Results of STAR (Safety Trial of Adalimumab in Rheumatoid Arthritis). The Journal of Rheumatology 2003;30:2563‐71. - PubMed
Keystone 2004 {published data only}
-
- Keystone EC, Kavanaugh AF, Sharp JT, Tannenbaum H, Hua Y, Teoh LS, et al. Radiographic, clinical, and functional outcomes of treatment with Adalimumab (a human anti‐tumor necrosis factor monoclonal antibody) in patients with active rheumatoid arthritis receiving concomitant methotrexate therapy. A randomized, placebo‐controlled, 52‐week trial. Arthritis & Rheumatism 2004;50:1400‐11. - PubMed
Rau 2004 {published data only}
-
- Rau R, Riel PLCM, Putte LBA, Kruger K, Schattenkirchner M, Allaart CF, et al. Rapid alleviation of signs and symptoms of rheumatoid arthritis with intravenous or subcutaneous administration of adalimumab in combination with methotrexate. Scandinavian Journal of Rheumatology 2004;33:145‐53. - PubMed
Van de Putte 2003 {published data only}
-
- Putte LBA, Rau R, Breedveld FC, Kalden JR, Malaise MG, Riel PLCM, et al. Efficacy and safety of the fully human anti‐tumor necrosis factor alpha monoclonal antibody adalimumab (D2E7) in DMARD refractory patients with rheumatoid arthritis: a 12 week, phase II study. Annals of the Rheumatic Diseases 2003;62:1168‐77. - PMC - PubMed
Van de Putte 2004 {published data only}
Weinblatt 2003 {published data only}
-
- Weinblatt ME, Keystone EC, Furst DE, Moreland LW, Weisman MH, Birbara CA, et al. Adalimumab, a fully human anti‐tumor necrosis factor alpha monoclonal antibody, for the treatment of rheumatoid arthritis in patients taking concomitant methotrexate. The ARMADA trial. Arthritis & Rheumatism 2003;48:33‐45. - PubMed
References to studies excluded from this review
Barrera 2002 {published data only}
-
- Barrera P, Maas A, Ede AE, Kiemeney BALM, Laan RFJM, Putte LBA, Riel PLCM. Drug survival, efficacy and toxicity of monotherapy with a full human anti‐tumor necrosis factor alpha antibody compared with methotrexate in long‐standing rheumatoid arthritis. Rheumatology 2002;41:430‐9. - PubMed
Den Broeder 2002a {published data only}
-
- Broeder A, Putte LBA, Rau R, Schattenkirchner M, Riel PLCM, Sander O, et al. A single dose, placebo controlled study of the fully human anti‐tumor necrosis factor alpha antibody Adalimumab (D2E7) in patients with rheumatoid arthritis. The Journal of Rheumatology 2002;29:2288‐98. - PubMed
Den Broeder 2002b {published data only}
-
- Broeder AA, Creemers MCW, Gestel AM, Riel PLCM. Dose tritation using the Disease Activity Score (DAS28) in rheumatoid arthritis patients treated with anti‐TNF‐alpha. Rheumatology 2002;41:638‐42. - PubMed
Den Broeder 2002c {published data only}
-
- Broeder AA, Joosten LAB, Saxne T, Heinegard D, Fenner H, Miltenburg AMM, et al. Long term anti‐tumor necrosis factor alpha monotherapy in rheumatoid arthritis: effect on radiological course and prognostic value of markers of cartlage turnover and endothelial activation. Annals of the Rheumatic Diseases 2002;61:311‐8. - PMC - PubMed
Den Broeder 2003 {published data only}
-
- Broeder A, Wanten GJA, Oyen WJG, Naber T, Riel PLCM, Barrera P. Neutrophil migration and production of reactive oxygen species during treatment with a fully human anti‐tumor necrosis factor alpha monoclonal antibody in patients with rheumatoid arthritis. The Journal of Rheumatology 2003;30:232‐7. - PubMed
Keystone 2003 {published data only}
-
- Keystone EC, Haraoui B, Bykerk VP. Role of Adalimumab in the treatment of early rheumatoid arthritis. Clinical and Experimental Rheumatology 2003;21 (suppl 31):S198‐S199. - PubMed
Schatenkirchner 1998 {published data only}
-
- Schattenkirchner M, Kruger K, Sander O, Rau R, Kroot EJ, Riel PLCM, et al. Efficacy and tolerability of weekly subcutaneous injections of the fully human anti‐TNF antibody D2E7 in patients with rheumatoid arthritis‐results of a phase I study (abstract). Arthritis & Rheumatism 1998; Vol. 41, issue suppl:S57.
Tjioe 2003 {published data only}
-
- Tjioe M, Gerritsen MJ, Broeder AA, Hooijdonk CA, Kroot EJ, Riel PLCM, et al. Adalimumab, a fully human anti‐TNF‐alpha monoclonal antibody, treatment does not influence experimental UV response in the skin of rheumatoid arthritis patients. Experimental Dermatology 2003;12:460‐5. - PubMed
Velagapudi 2004 {published data only}
-
- Velagapudi RB, Noertershuser PA, Awni W, Grannenman RG, Chartash E. Adalimumab (Humira) 40 mg every other week plus methotrexate in patients with rheumatoid arthritis provides stable serum concentrations and sustaines efficacy over 1 year. Annals of the Rheumatic Diseases 2004; Vol. 63, issue suppl I:267.
Weisman 2003 {published data only}
-
- Weissman MH, Moreland LW, Furst DE, Weinblatt ME, Keystone EC, Paulus HE, et al. Efficacy, pharmacokinetic, and safety assessment of Adalimumab, a fully human anti‐tumor necrosis factor‐alpha monoclonal antibody, in adults with rheumatoid arthritis receiving concomitant methotrexate: a pilot study. Clinical Therapeutics 2003;25:1700‐21. - PubMed
Additional references
Arnett 1988
-
- Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, et al. The American Rheumatism Association revised criteria for the classification of rheumatoid arthrtitis. Arthritis & Rheumatism 1988;31:315‐24. - PubMed
Blumenauer 2003a
Blumenauer 2003b
-
- Blumenauer B, Judd M, Cranney A, Burls A, Coyle D, Hochberg M, Tugwell P, Wells G. Etanercept for the treatment of rheumatoid arthritis.. Cochrane Database of Systematic Reviews 2003, Issue 4. [Issue 3. Art. No.: CD004525. DOI: 10.1002/14651858.CD004525. Issue 3. Art. No.: CD004525. DOI: 10.1002/14651858.CD004525. Issue 3. Art. No.: CD004525. DOI: 10.1002/14651858.CD004525.] - PubMed
Cates 2003
-
- Cates, C. EBM website. URL:http://www.nntonline.net/ 2003.
Clarke 2001
-
- Clarke M, Oxman AD, editors. Cochrane Review Handbook 4.1.2. (update March 2001).. The Cochrane Library, Issue 2, 2001. 2001.
Felson 1995
-
- Felson DT, Anderson JJ, Boers M, Bombardier C, Furst D, Goldsmith D, et al. American College of Rheumatology preliminary definition of improvement in rheumatoid arthritis. Arthritis & Rheumatism 1995;38:727‐35. - PubMed
Jadad 1996
-
- Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding neccesary?. Controlled Clinical trials 1996;17:1‐12. - PubMed
Tugwell 2004
-
- Tugwell P, Shea B, Boers M, Brooks P, Simon L, Strand V, Wells G (editors). Evidence‐based Rheumatology. London: BMJ Books, 2004.
van der Heijde 1993
-
- Heijde DM, Hof M, Riel PL, Putte LB. Development of a disease activity score based on judgment in clinical practice by rheumatologists. The Journal of Rheumatology 1993;20:579‐81. - PubMed
Van Gestel 1996
-
- Gestel AM, Prevoo ML, Hof MA, Rijswijk MH, Putte LB, Riel PL. Development and validation of the European League Against Rheumatism response criteria for rheumaotid arthritis. Comparison with the preliminary American College of Rheumatology and the Worl Health Organisation/International League Against Rheumatism criteria. Arthritis & Rheumatism 1996;39:34‐40. - PubMed
Verhagen 1998
-
- Verhagen AP, Vet HC, Bie RA, Kessels AG, Boers M, Bouter LM, Knipschild PG. The Delphi list: a criteria list for quality assessment of randomized clinical trials for conducting systematc review developed by Delphi consensus. The Journal of Clinical Epidemiology 1998;51:1235‐41. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous