

Treatment of uncomplicated reflux disease
- PMID: 16038023
- PMCID: PMC4434651
- DOI: 10.3748/wjg.v11.i28.4291
Treatment of uncomplicated reflux disease
Abstract
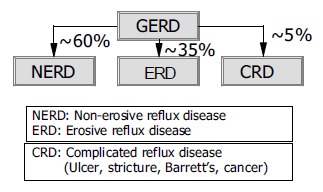
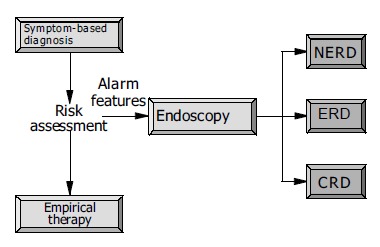
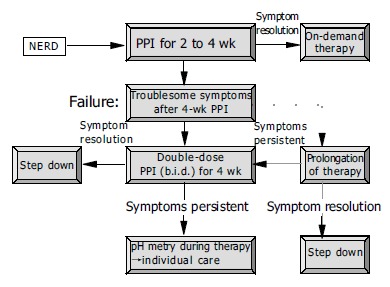
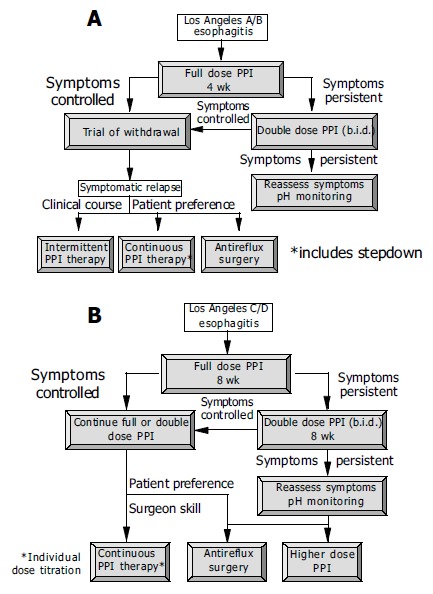
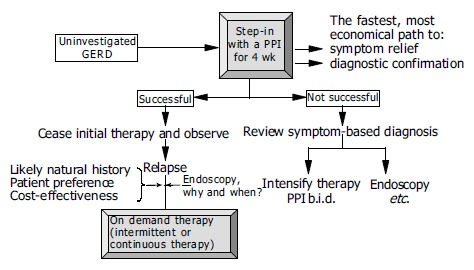
Uncomplicated reflux disease comprises the non-erosive reflux disease (NERD) and erosive reflux disease (ERD). The objectives of treatment are the adequate control of symptoms with restoration of quality of life, healing of lesions and prevention of relapse. Treatment of NERD consists in the administration of proton pump inhibitors (PPI) for 2-4 wk, although patients with NERD show an overall poorer response to PPI treatment than patients with ERD owing to the fact that patients with NERD do not form a pathophysiologically homogenous group. For long-term management on-demand treatment with a PPI is probably the best option. In patients with ERD, therapy with a standard dose PPI for 4-8 wk is always recommended. Long-term treatment of ERD is applied either intermittently or as continuous maintenance treatment with an attempt to reduce the daily dosage of the PPI (step-down principle). In selected patients requiring long-term PPI treatment, antireflux surgery is an alternative option. In patients with troublesome reflux symptoms and without alarming features empirical PPI therapy is another option for initial management. Therapy should be withdrawn after initial success. In the case of relapse, the long-term care depends on a careful risk assessment and the response to PPI therapy.
Figures
References
-
- Locke GR, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ. Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology. 1997;112:1448–1456. - PubMed
-
- Quigley EM. Non-erosive reflux disease: part of the spectrum of gastro-oesophageal reflux disease, a component of functional dyspepsia, or both? Eur J Gastroenterol Hepatol. 2001;13 Suppl 1:S13–S18. - PubMed
-
- Fass R, Ofman JJ. Gastroesophageal reflux disease--should we adopt a new conceptual framework? Am J Gastroenterol. 2002;97:1901–1909. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
