

Prevalence of male and female sexual dysfunction is high following surgery for rectal cancer
- PMID: 16041212
- PMCID: PMC1357727
- DOI: 10.1097/01.sla.0000171299.43954.ce
Prevalence of male and female sexual dysfunction is high following surgery for rectal cancer
Abstract
Objective: To measure sexual function and quality of life (QOL) after rectal cancer treatment.
Summary background data: Previous studies on sexual function after rectal cancer treatment have focused on males and have not used validated instruments.
Methods: Patients undergoing curative rectal cancer surgery from 1980 to 2003 were administered a questionnaire, including the Female Sexual Function Index (FSFI) or International Index of Erectile Function (IIEF), and the EORTC QLQ-C30/CR-38. Multiple logistic regression was used to test associations of clinical factors with outcomes.
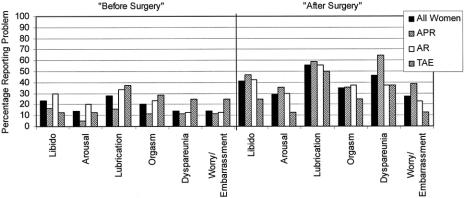
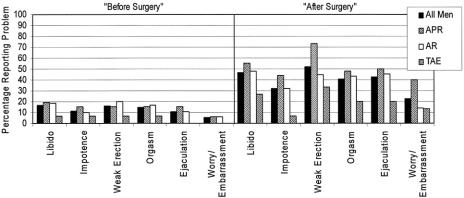
Results: Eighty-one women (81.0%) and 99 men (80.5%) returned the questionnaire; 32% of women and 50% of men are sexually active, compared with 61% and 91% preoperatively (P < 0.04); 29% of women and 45% of men reported that "surgery made their sexual lives worse." Mean (SD) FSFI and IIEF scores were 17.5 (11.9) and 29.3 (22.8). Specific sexual problems in women were libido 41%, arousal 29%, lubrication 56%, orgasm 35%, and dyspareunia 46%, and in men libido 47%, impotence 32%, partial impotence 52%, orgasm 41%, and ejaculation 43%. Both genders reported a negative body image. Patients seldom remembered discussing sexual risks preoperatively and seldom were treated for dysfunction. Current age (P < 0.001), surgical procedure (P = 0.003), and preoperative sexual activity (P = 0.001) were independently associated with current sexual activity. Gender (male, P = 0.014), surgical procedure (P = 0.005), and radiation therapy (P = 0.0001) were independently associated with the outcome "surgery made sexual life worse." Global QOL scores were high.
Conclusions: Sexual problems after surgery for rectal cancer are common, multifactorial, inadequately discussed, and untreated. Therefore, sexual dysfunction should be discussed with rectal cancer patients, and efforts to prevent and treat it should be increased.
Figures
Comment in
-
Perioperative radiation for rectal cancer and sexual dysfunction after TME: cause and effect?Ann Surg. 2007 Jan;245(1):155. doi: 10.1097/01.sla.0000250943.83211.f1. Ann Surg. 2007. PMID: 17197984 Free PMC article. No abstract available.
References
-
- Sprangers MA, Taal BG, Aaronson NK, et al. Quality of life in colorectal cancer: stoma vs. nonstoma patients. Dis Colon Rectum. 1995;38:361–369. - PubMed
-
- Havenga K, Maas CP, DeRuiter MC, et al. Avoiding long-term disturbance to bladder and sexual function in pelvic surgery, particularly with rectal cancer. Semin Surg Oncol. 2000;18:235–243. - PubMed
-
- Camilleri-Brennan J, Steele RJ. Quality of life after treatment for rectal cancer. Br J Surg. 1998;85:1036–1043. - PubMed
-
- Masui H, Ike H, Yamaguchi S, et al. Male sexual function after autonomic nerve-preserving operation for rectal cancer. Dis Colon Rectum. 1996;39:1140–1145. - PubMed
-
- Havenga K, Enker WE, McDermott K, et al. Male and female sexual and urinary function after total mesorectal excision with autonomic nerve preservation for carcinoma of the rectum. J Am Coll Surg. 1996;182:495–502. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
