

Left hepatic trisectionectomy for hepatobiliary malignancy: results and an appraisal of its current role
- PMID: 16041218
- PMCID: PMC1357733
- DOI: 10.1097/01.sla.0000171304.70678.11
Left hepatic trisectionectomy for hepatobiliary malignancy: results and an appraisal of its current role
Abstract
Objective: To analyze results of 70 patients undergoing left hepatic trisectionectomy and to clarify its current role.
Summary background data: Left hepatic trisectionectomy remains a complicated hepatectomy, and few reports have described the long-term results of the procedure.
Methods: Short-term and long-term outcomes of 70 consecutive patients who underwent left hepatic trisectionectomy from January 1993 to February 2004 were analyzed.
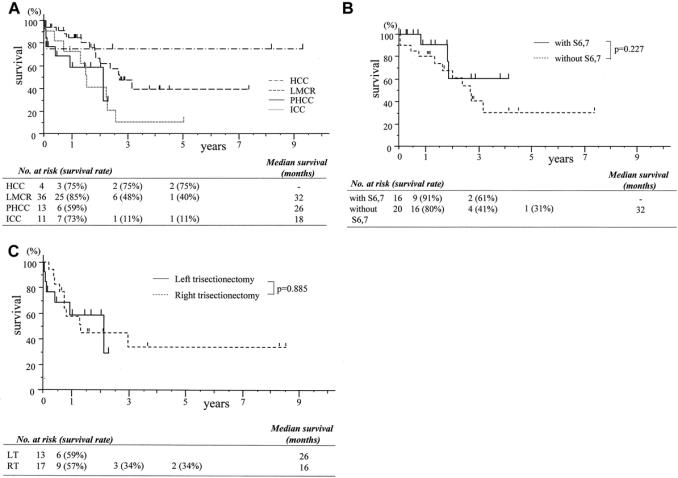
Results: Of the 70 patients, 36 had colorectal liver metastasis, 24 had cholangiocarcinoma, 4 had hepatocellular carcinoma, and the remaining 6 had other tumors. Overall morbidity, 30-day and 90-day mortality rates were 46%, 7%, and 9%, respectively. Multivariate analysis disclosed that preoperative jaundice and intraoperative blood transfusion were positive independent predictors for postoperative morbidity; however, there were no independent predictors for postoperative mortality. Postoperative morbidity (87% versus 35%, P < 0.001) and mortality (20% versus 5%, P = 0.108) were observed more frequently in patients with preoperative obstructive jaundice than in those without jaundice. Each survival according to tumor type was acceptable compared with reported survivals. Survival for patients with colorectal liver metastasis undergoing left hepatic trisectionectomy with concomitant partial resection of the remnant liver was similar to those without this concomitant procedure. This concomitant procedure was not associated with postoperative morbidity and mortality.
Conclusions: Left hepatic trisectionectomy remains a challenging procedure. Preoperative obstructive jaundice considerably increases perioperative risk. Concomitant partial resection of the remaining liver appears to be safe and offers the potential for cure in patients with colorectal metastasis affecting all liver segments.
Figures

References
-
- The terminology committee of the IHPBA: the Brisbane 2000 terminology of hepatic anatomy and resections. HPB. 2000;2:333–339. - PubMed
-
- Blumgart LH, Baer HU, Czerniak A, et al. Extended left hepatectomy: technical aspects of an evolving procedure. Br J Surg. 1993;80:903–906. - PubMed
-
- Huguet C, Stipa F, Gavelli A. Extended left hepatectomy with vascular exclusion. J Am Coll Surg. 1994;178:288–292. - PubMed
-
- Makuuchi M, Thai BL, Takayasu K, et al. Preoperative portal embolization to increase safety of major hepatectomy for hilar bile duct carcinoma: a preliminary report. Surgery. 1990;107:521–527. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
