

Impact of an electronic medical record on diabetes quality of care
- PMID: 16046561
- PMCID: PMC1466905
- DOI: 10.1370/afm.327
Impact of an electronic medical record on diabetes quality of care
Abstract
Purpose: This study was designed to evaluate the impact of electronic medical record (EMR) implementation on quality of diabetes care.
Methods: We conducted a 5-year longitudinal study of 122 adults with diabetes mellitus at an intervention (EMR) clinic and a comparison (non-EMR) clinic. Clinics had similarly trained primary care physicians, similar patient populations, and used a common diabetes care guideline that emphasized the importance of glucose control. The EMR provided basic decision support, including prompts and reminders for diabetes care. Preintervention and postintervention frequency of testing for glycated hemoglobin (HbA1c) and low-density lipoprotein (LDL) levels were compared with and without adjustment for patient age, sex, comorbidity, and baseline HbA1c level.
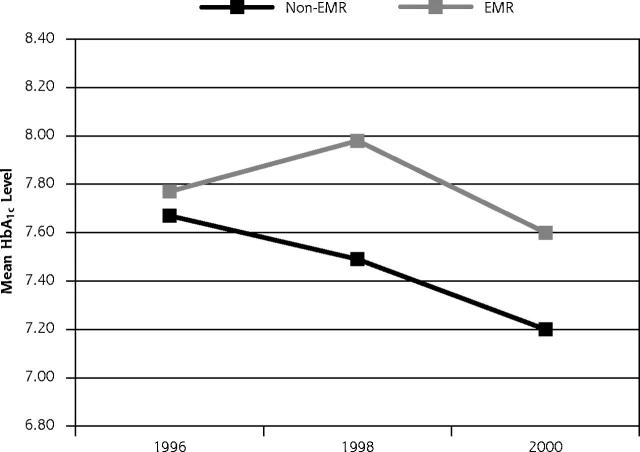
Results: Frequency of HbA1c tests increased at the EMR clinic compared with the frequency at the non-EMR clinic (P < .001). HbA1c levels improved in both clinics (P < .05) with no significant differences between clinics 2 years (P = .10) or 4 years (P = .27) after EMR implementation. Similar results were observed for LDL levels.
Conclusions: In this controlled study, EMR use led to an increased number of HbA1c and LDL tests but not to better metabolic control. If EMRs are to fulfill their promise as care improvement tools, improved implementation strategies and more sophisticated clinical decision support may be needed.
Figures
References
-
- Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS, Koplan JP. The continuing epidemics of obesity and diabetes in the United States. JAMA. 2001;286:1195–1200. - PubMed
-
- Marrero DG. Current effectiveness of diabetes health care in the United States. Diabetes Rev. 1994;2:292–309.
-
- Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC, National Academy Press; 2001.
-
- Institute of Medicine (IOM). To err is human: building a safer health system. Washington, DC: National Academy Press; 2000
-
- O’Connor PJ, Solberg LI, Baird M. The future of primary care. The enhanced primary care model. J Fam Pract. 1998;47:62–67. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical