

Symptomatic severity of PRIME-MD diagnosed episodes of panic and generalized anxiety disorder in primary care
- PMID: 16050857
- PMCID: PMC1490149
- DOI: 10.1111/j.1525-1497.2005.0120.x
Symptomatic severity of PRIME-MD diagnosed episodes of panic and generalized anxiety disorder in primary care
Abstract
Background: Panic disorder (PD) and generalized anxiety disorder (GAD) are often unrecognized by primary care physicians (PCPs). The Primary Care Evaluation of Mental Disorders (PRIME-MD) has been used as a case-finding instrument for depression. Yet, little is known on its usefulness as a case-finding tool for anxiety disorders within the context of a clinical trial.
Objective: To examine the: (1) completion rate of the PRIME-MD by patients approached to enroll in a treatment study for PD and GAD; (2) distribution of anxiety diagnoses generated; (3) severity of PD and GAD episodes thus identified; and (4) level of PCPs' agreement with these diagnoses.
Design: Cross-sectional interview.
Patients: Individuals aged 18 to 64 who presented for care at 4 primary care practices.
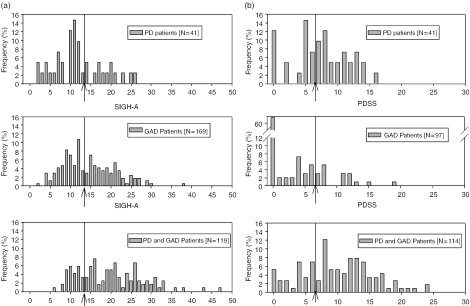
Measurements: The PRIME-MD, Structured Interview Guide for the Hamilton Anxiety Rating Scale (SIGH-A), and the Panic Disorder Severity Scale (PDSS).
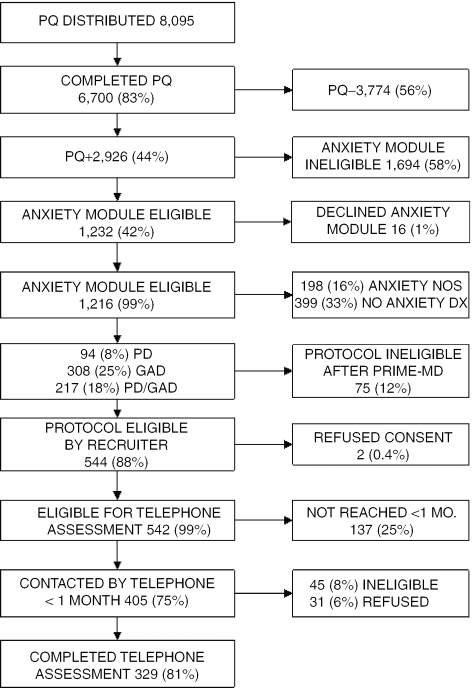
Results: Of the 6,700 patients who completed the PRIME-MD Patient Questionnaire (PQ), 2,926 (44%) screened positive for an anxiety disorder, and 1,216 (42%) met preliminary study eligibility and consented to the PRIME-MD Anxiety Module. Of these, 619 (51%) had either GAD (308), PD (94), or both (217) disorders. Later, 329 completed a telephone interview. Of these, 59% with GAD and 68% with PD reported moderate or greater levels of anxiety symptoms on the SIGH-A and PDSS, respectively, and PCPs agreed with the PRIME-MD diagnosis for 98% of these patients.
Conclusions: The PRIME-MD can efficiently screen patients for PD and GAD. Although patients thus identified endorse a wide range of anxiety symptoms, PCPs often agree with the diagnosis.
Figures
References
-
- Stein MB, Barrett-Connor E. Quality of life in older adults receiving medications for anxiety, depression, or insomnia. findings from a community-based study Am J Geriatric Psychiatry. 2002;10:568–574. - PubMed
-
- Lane D, Carroll D, Ring C, Beevers DG, Lip GY. Mortality and quality of life 12 months after myocardial infarction. effects of depression and anxiety Psychosomatic Med. 2001;63:221–230. - PubMed
-
- Cass AR, Volk RJ, Nease DE., Jr Health-related quality of life in primary care patients with recognized and unrecognized mood and anxiety disorders. Int J Psychiatry Med. 1999;29:293–309. - PubMed
-
- Greenberg PE, Sisitsky T, Kessler RC, et al. The economic burden of anxiety disorders in the 1990s. J Clin Psychiatry. 1999;60:427–435. - PubMed
-
- Regier DA, Boyd JH, Burke JD, Jr, et al. One-month prevalence of mental disorders in the United States. Based on five epidemiologic catchment area sites. Arch Gen Psychiatry. 1988;45:977–986. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous