

Trends in antibiotic prescribing for adults in the United States--1995 to 2002
- PMID: 16050877
- PMCID: PMC1490171
- DOI: 10.1111/j.1525-1497.2005.0148.x
Trends in antibiotic prescribing for adults in the United States--1995 to 2002
Abstract
Context: The impact of national efforts to limit antibiotic prescribing has not been fully evaluated.
Objectives: To analyze trends in outpatient visits associated with antibiotic prescription for U.S. adults.
Design: Cross-sectional study of data (1995 to 2002) from the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey.
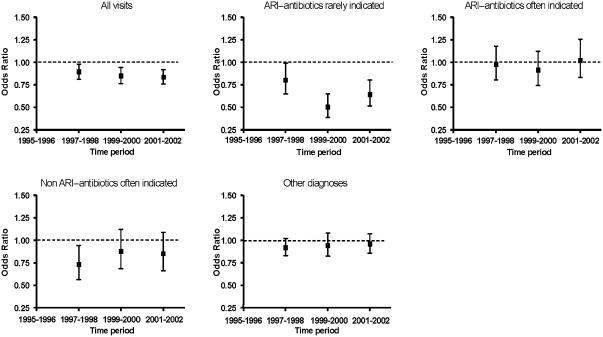
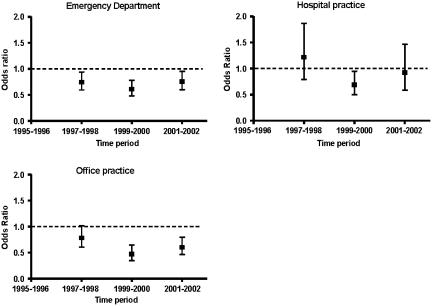
Participants: Adults > or =18 years with an outpatient visit to an office- or hospital-based medical practice or to an emergency department. All visits were classified into 1 of 4 diagnostic categories: (1) acute respiratory infection (ARI)-antibiotics rarely indicated, (2) ARI-antibiotics often indicated, (3) nonrespiratory infection-antibiotics often indicated, and (4) all others.
Measurements: Trends in: (1) Proportion of outpatient visits associated with an antibiotic prescription; (2) proportion of antibiotic prescriptions that were broad spectrum; and (3) number of visits and antibiotic prescriptions per 1,000 U.S. adults > or =18 years of age.
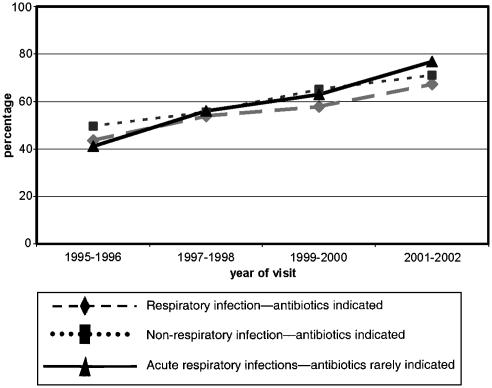
Results: From 1995-1996 to 2001-2002, the proportion of all outpatient visits that generated an antibiotic prescription decreased from 17.9% to 15.3% (adjusted odds ratio [OR] 0.84, 95 % confidence interval [CI] 0.76 to 0.92). The entire reduction was because of a decrease in antibiotic prescriptions associated with visits for ARIs where antibiotics are rarely indicated from 59.9% to 49.1% (adjusted OR 0.64 95% CI 0.51 to 0.80). However, the proportion of prescribed antibiotics for these visits that were classified as broad-spectrum antibiotic prescription increased from 41.0% to 76.8%. Overall outpatient visits increased from 1693 to 1986 per 1,000 adults over the 8 years studied, but associated antibiotic prescriptions changed little, from 302 to 304 per 1,000 adults.
Conclusion: During the study period, outpatient antibiotic prescribing for respiratory infections where antibiotics are rarely indicated has declined, while the proportion of broad-spectrum antibiotics prescribed for these diagnoses has increased significantly. This trend resulted in a 15% decline in the total proportion of outpatient visits in which antibiotics were prescribed. However, because outpatient visits increased 17% over this time period, the population burden of outpatient antibiotic prescriptions changed little.
Figures
References
-
- Arroll B, Kenealy T. Antibiotics for the common cold. Cochrane Database Syst Rev. 2002:CD000247. - PubMed
-
- Thomas MG, Arroll B. “Just say no”—reducing the use of antibiotics for colds, bronchitis and sinusitis. N Z Med J. 2000;113:287–9. - PubMed
-
- Bertino JS. Cost burden of viral respiratory infections: issues for formulary decision makers. Am J Med. 2002;112(suppl 6A):42S–9S. - PubMed
-
- McCaig LF, Hughes JM. Trends in antimicrobial drug prescribing among office-based physicians in the United States. JAMA. 1995;273:214–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical